

Benefits in radical mastectomy protocol: a randomized trial evaluating the use of regional anesthesia
- PMID: 29777144
- PMCID: PMC5959858
- DOI: 10.1038/s41598-018-26273-z
Benefits in radical mastectomy protocol: a randomized trial evaluating the use of regional anesthesia
Abstract
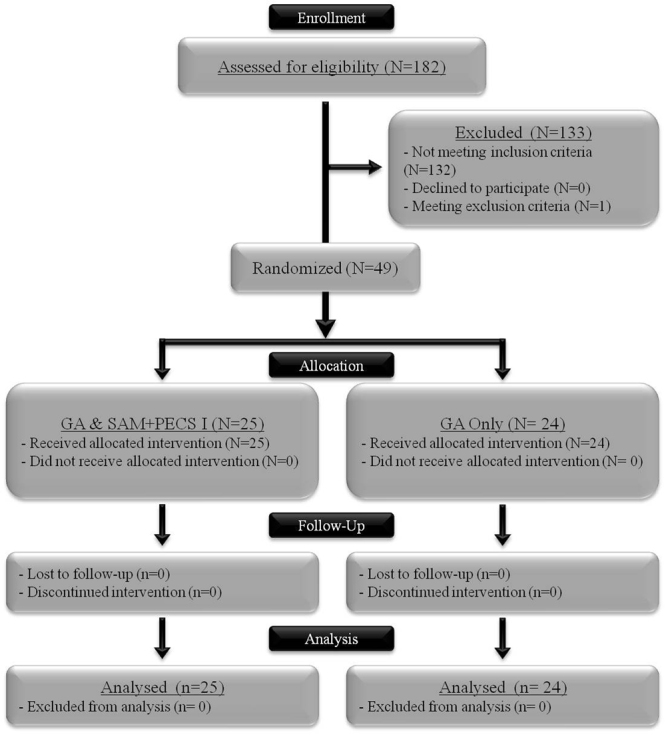
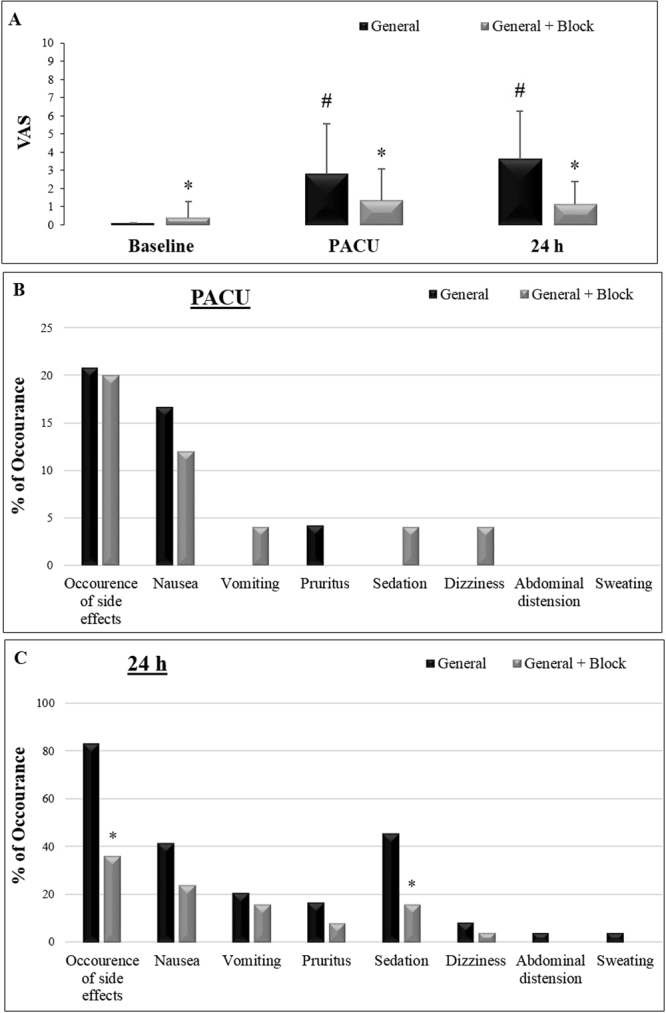
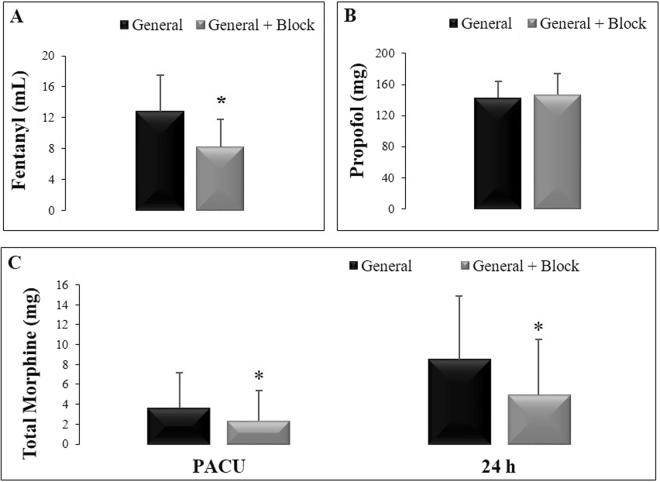
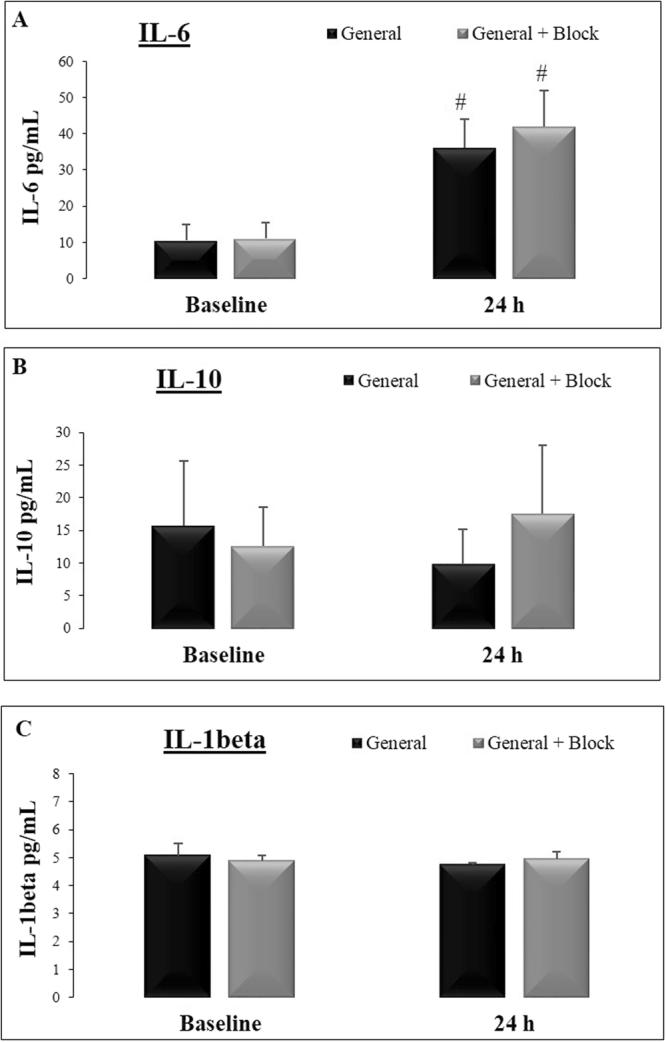
Surgery is the first-line treatment for early, localized, or operable breast cancer. Regional anesthesia during mastectomy may offer the prevention of postoperative pain. One potential protocol is the combination of serratus anterior plane block (SAM block) with pectoral nerve block I (PECS I), but the results and potential benefits are limited. Our study compared general anesthesia with or without SAM block + PECS I during radical mastectomy with axillary node dissection and breast reconstruction using evaluations of pain, opioid consumption, side effects and serum levels of interleukin (IL)-1beta, IL-6 and IL-10. This is a prospective, randomized controlled trial. Fifty patients were randomized to general anesthesia only or general anesthesia associated with SAM block + PECS I (25 per group). The association of SAM block + PECS I with general anesthesia reduced intraoperative fentanyl consumption, morphine use and visual analog pain scale scores in the post-anesthetic care unit (PACU) and at 24 h after surgery. In addition, the anesthetic protocol decreased side effects and sedation 24 h after surgery compared to patients who underwent general anesthesia only. IL-6 levels increased after the surgery compared to baseline levels in both groups, and no differences in IL-10 and IL-1 beta levels were observed. Our protocol improved the outcomes of mastectomy, which highlight the importance of improving mastectomy protocols and focusing on the benefits of regional anesthesia.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- World Health Organization. Global health estimates (WHO, 2013).
-
- PDQ Adult Treatment Editorial Board. Breast cancer treatment (PDQ®): patient version, http://www.ncbi.nlm.nih.gov/books/NBK65969/PubMed (2002). - PubMed
-
- Smith HS, Wu SX. Persistent pain after breast cancer treatment. Ann. Palliat. Med. 2012;1:182–194. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
