

Cerebral microbleeds and intracranial haemorrhage risk in patients anticoagulated for atrial fibrillation after acute ischaemic stroke or transient ischaemic attack (CROMIS-2): a multicentre observational cohort study
- PMID: 29778365
- PMCID: PMC5956310
- DOI: 10.1016/S1474-4422(18)30145-5
Cerebral microbleeds and intracranial haemorrhage risk in patients anticoagulated for atrial fibrillation after acute ischaemic stroke or transient ischaemic attack (CROMIS-2): a multicentre observational cohort study
Erratum in
-
Corrections.Lancet Neurol. 2018 Jul;17(7):578. doi: 10.1016/S1474-4422(18)30205-9. Epub 2018 May 26. Lancet Neurol. 2018. PMID: 29807814 Free PMC article. No abstract available.
Abstract
Background: Cerebral microbleeds are a potential neuroimaging biomarker of cerebral small vessel diseases that are prone to intracranial bleeding. We aimed to determine whether presence of cerebral microbleeds can identify patients at high risk of symptomatic intracranial haemorrhage when anticoagulated for atrial fibrillation after recent ischaemic stroke or transient ischaemic attack.
Methods: Our observational, multicentre, prospective inception cohort study recruited adults aged 18 years or older from 79 hospitals in the UK and one in the Netherlands with atrial fibrillation and recent acute ischaemic stroke or transient ischaemic attack, treated with a vitamin K antagonist or direct oral anticoagulant, and followed up for 24 months using general practitioner and patient postal questionnaires, telephone interviews, hospital visits, and National Health Service digital data on hospital admissions or death. We excluded patients if they could not undergo MRI, had a definite contraindication to anticoagulation, or had previously received therapeutic anticoagulation. The primary outcome was symptomatic intracranial haemorrhage occurring at any time before the final follow-up at 24 months. The log-rank test was used to compare rates of intracranial haemorrhage between those with and without cerebral microbleeds. We developed two prediction models using Cox regression: first, including all predictors associated with intracranial haemorrhage at the 20% level in univariable analysis; and second, including cerebral microbleed presence and HAS-BLED score. We then compared these with the HAS-BLED score alone. This study is registered with ClinicalTrials.gov, number NCT02513316.
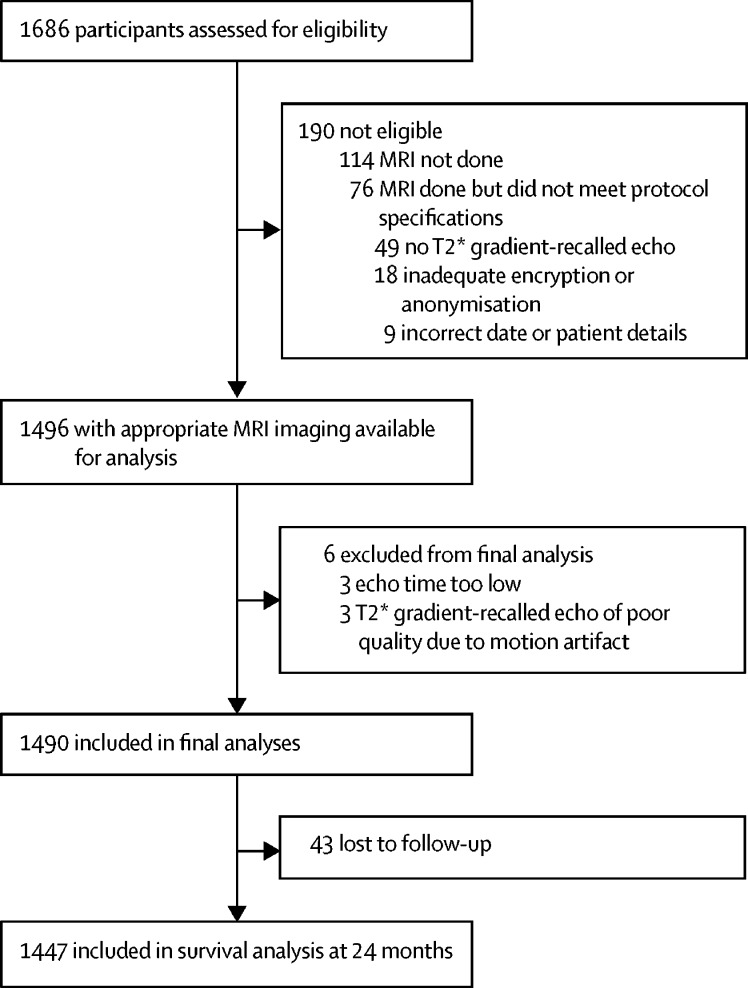
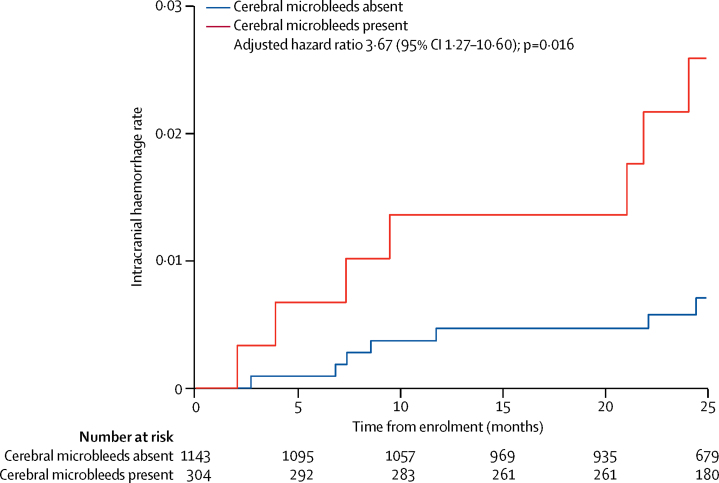
Findings: Between Aug 4, 2011, and July 31, 2015, we recruited 1490 participants of whom follow-up data were available for 1447 (97%), over a mean period of 850 days (SD 373; 3366 patient-years). The symptomatic intracranial haemorrhage rate in patients with cerebral microbleeds was 9·8 per 1000 patient-years (95% CI 4·0-20·3) compared with 2·6 per 1000 patient-years (95% CI 1·1-5·4) in those without cerebral microbleeds (adjusted hazard ratio 3·67, 95% CI 1·27-10·60). Compared with the HAS-BLED score alone (C-index 0·41, 95% CI 0·29-0·53), models including cerebral microbleeds and HAS-BLED (0·66, 0·53-0·80) and cerebral microbleeds, diabetes, anticoagulant type, and HAS-BLED (0·74, 0·60-0·88) predicted symptomatic intracranial haemorrhage significantly better (difference in C-index 0·25, 95% CI 0·07-0·43, p=0·0065; and 0·33, 0·14-0·51, p=0·00059, respectively).
Interpretation: In patients with atrial fibrillation anticoagulated after recent ischaemic stroke or transient ischaemic attack, cerebral microbleed presence is independently associated with symptomatic intracranial haemorrhage risk and could be used to inform anticoagulation decisions. Large-scale collaborative observational cohort analyses are needed to refine and validate intracranial haemorrhage risk scores incorporating cerebral microbleeds to identify patients at risk of net harm from oral anticoagulation.
Funding: The Stroke Association and the British Heart Foundation.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Balancing risks versus benefits of anticoagulants in stroke prevention.Lancet Neurol. 2018 Jun;17(6):487-488. doi: 10.1016/S1474-4422(18)30164-9. Epub 2018 May 16. Lancet Neurol. 2018. PMID: 29778352 No abstract available.
References
-
- Rockson SG, Albers GW. Comparing the guidelines: anticoagulation therapy to optimize stroke prevention in patients with atrial fibrillation. J Am Coll Cardiol. 2004;43:929–935. - PubMed
-
- Dogliotti A, Paolasso E, Giugliano RP. Current and new oral antithrombotics in non-valvular atrial fibrillation: a network meta-analysis of 79 808 patients. Heart. 2014;100:396–405. - PubMed
-
- Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857–867. - PubMed
-
- Dowlatshahi D, Butcher KS, Asdaghi N. Poor prognosis in warfarin-associated intracranial hemorrhage despite anticoagulation reversal. Stroke. 2012;43:1812–1817. - PubMed
-
- Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010;138:1093–1100. - PubMed
