

Risk-adapted therapy for young children with medulloblastoma (SJYC07): therapeutic and molecular outcomes from a multicentre, phase 2 trial
- PMID: 29778738
- PMCID: PMC6078206
- DOI: 10.1016/S1470-2045(18)30204-3
Risk-adapted therapy for young children with medulloblastoma (SJYC07): therapeutic and molecular outcomes from a multicentre, phase 2 trial
Abstract
Background: Young children with medulloblastoma have a poor overall survival compared with older children, due to use of radiation-sparing therapy in young children. Radiotherapy is omitted or reduced in these young patients to spare them from debilitating long-term side-effects. We aimed to estimate event-free survival and define the molecular characteristics associated with progression-free survival in young patients with medulloblastoma using a risk-stratified treatment strategy designed to defer, reduce, or delay radiation exposure.
Methods: In this multicentre, phase 2 trial, we enrolled children younger than 3 years with newly diagnosed medulloblastoma at six centres in the USA and Australia. Children aged 3-5 years with newly diagnosed, non-metastatic medulloblastoma without any high-risk features were also eligible. Eligible patients were required to start therapy within 31 days from definitive surgery, had a Lansky performance score of at least 30, and did not receive previous radiotherapy or chemotherapy. Patients were stratified postoperatively by clinical and histological criteria into low-risk, intermediate-risk, and high-risk treatment groups. All patients received identical induction chemotherapy (methotrexate, vincristine, cisplatin, and cyclophosphamide), with high-risk patients also receiving an additional five doses of vinblastine. Induction was followed by risk-adapted consolidation therapy: low-risk patients received cyclophosphamide (1500 mg/m2 on day 1), etoposide (100 mg/m2 on days 1 and 2), and carboplatin (area under the curve 5 mg/mL per min on day 2) for two 4-week cycles; intermediate-risk patients received focal radiation therapy (54 Gy with a clinical target volume of 5 mm over 6 weeks) to the tumour bed; and high-risk patients received chemotherapy with targeted intravenous topotecan (area under the curve 120-160 ng-h/mL intravenously on days 1-5) and cyclophosphamide (600 mg/m2 intravenously on days 1-5). After consolidation, all patients received maintenance chemotherapy with cyclophosphamide, topotecan, and erlotinib. The coprimary endpoints were event-free survival and patterns of methylation profiling associated with progression-free survival. Outcome and safety analyses were per protocol (all patients who received at least one dose of induction chemotherapy); biological analyses included all patients with tissue available for methylation profiling. This trial is registered with ClinicalTrials.gov, number NCT00602667, and was closed to accrual on April 19, 2017.
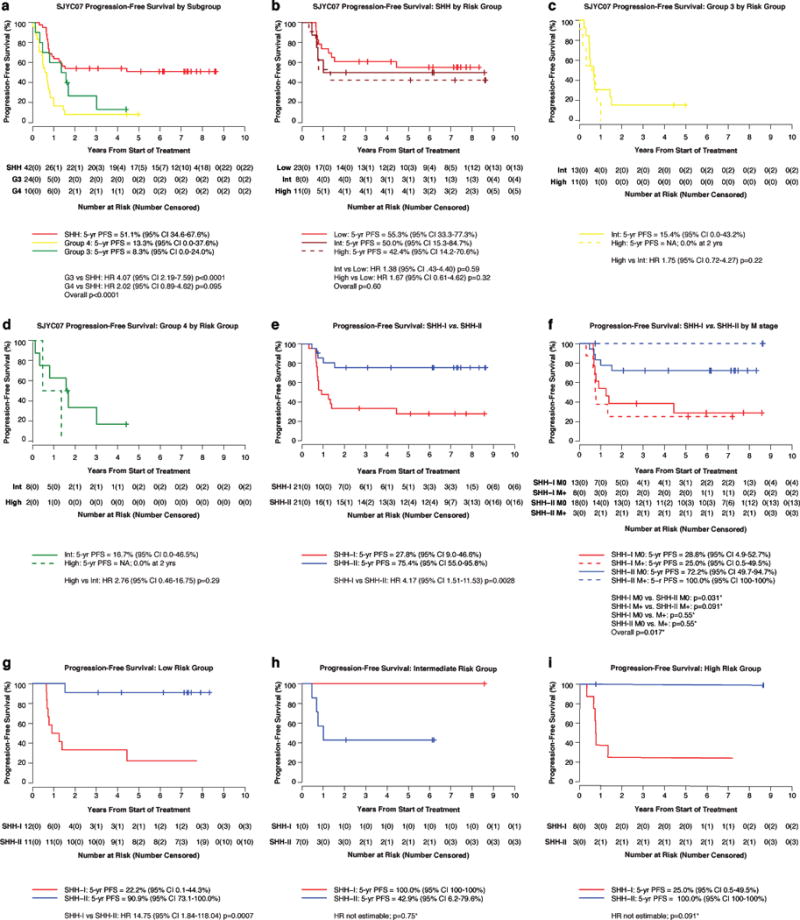
Findings: Between Nov 27, 2007, and April 19, 2017, we enrolled 81 patients with histologically confirmed medulloblastoma. Accrual to the low-risk group was suspended after an interim analysis on Dec 2, 2015, when the 1-year event-free survival was estimated to be below the stopping rule boundary. After a median follow-up of 5·5 years (IQR 2·7-7·3), 5-year event-free survival was 31·3% (95% CI 19·3-43·3) for the whole cohort, 55·3% (95% CI 33·3-77·3) in the low-risk cohort (n=23) versus 24·6% (3·6-45·6) in the intermediate-risk cohort (n=32; hazard ratio 2·50, 95% CI 1·19-5·27; p=0·016) and 16·7% (3·4-30·0) in the high-risk cohort (n=26; 3·55, 1·66-7·59; p=0·0011; overall p=0·0021). 5-year progression-free survival by methylation subgroup was 51·1% (95% CI 34·6-67·6) in the sonic hedgehog (SHH) subgroup (n=42), 8·3% (95% CI 0·0-24·0%) in the group 3 subgroup (n=24), and 13·3% (95% CI 0·0-37·6%) in the group 4 subgroup (n=10). Within the SHH subgroup, two distinct methylation subtypes were identified and named iSHH-I and iSHH-II. 5-year progression-free survival was 27·8% (95% CI 9·0-46·6; n=21) for iSHH-I and 75·4% (55·0-95·8; n=21) for iSHH-II. The most common adverse events were grade 3-4 febrile neutropenia (48 patients [59%]), neutropenia (21 [26%]), infection with neutropenia (20 [25%]), leucopenia (15 [19%]), vomiting (15 [19%]), and anorexia (13 [16%]). No treatment-related deaths occurred.
Interpretation: The risk-adapted approach did not improve event-free survival in young children with medulloblastoma. However, the methylation subgroup analyses showed that the SHH subgroup had improved progression-free survival compared with the group 3 subgroup. Moreover, within the SHH subgroup, the iSHH-II subtype had improved progression-free survival in the absence of radiation, intraventricular chemotherapy, or high-dose chemotherapy compared with the iSHH-I subtype. These findings support the development of a molecularly driven, risk-adapted, treatment approach in future trials in young children with medulloblastoma.
Funding: American Lebanese Syrian Associated Charities, St Jude Children's Research Hospital, NCI Cancer Center, Alexander and Margaret Stewart Trust, Sontag Foundation, and American Association for Cancer Research.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
All other authors declare no competing financial interests
Figures




Comment in
-
Medulloblastoma in infants: the never-ending challenge.Lancet Oncol. 2018 Jun;19(6):720-721. doi: 10.1016/S1470-2045(18)30278-X. Epub 2018 May 16. Lancet Oncol. 2018. PMID: 29778736 No abstract available.
-
Infant medulloblastoma - learning new lessons from old strata.Nat Rev Clin Oncol. 2018 Nov;15(11):659-660. doi: 10.1038/s41571-018-0071-6. Nat Rev Clin Oncol. 2018. PMID: 30030473 No abstract available.
References
-
- Gajjar A, Chintagumpala M, Ashley D, Kellie S, Kun LE, Merchant TE, et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): long-term results from a prospective, multicentre trial. The Lancet Oncology. 2006;7(10):813–20. - PubMed
-
- Packer RJ, Gajjar A, Vezina G, Rorke-Adams L, Burger PC, Robertson PL, et al. Phase III study of craniospinal radiation therapy followed by adjuvant chemotherapy for newly diagnosed average-risk medulloblastoma. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2006;24(25):4202–8. - PubMed
-
- Dhall G, Grodman H, Ji L, Sands S, Gardner S, Dunkel IJ, et al. Outcome of children less than three years old at diagnosis with non-metastatic medulloblastoma treated with chemotherapy on the “Head Start” I and II protocols. Pediatric blood & cancer. 2008;50(6):1169–75. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
