

Defining Host Responses during Systemic Bacterial Infection through Construction of a Murine Organ Proteome Atlas
- PMID: 29778837
- PMCID: PMC7868092
- DOI: 10.1016/j.cels.2018.04.010
Defining Host Responses during Systemic Bacterial Infection through Construction of a Murine Organ Proteome Atlas
Abstract
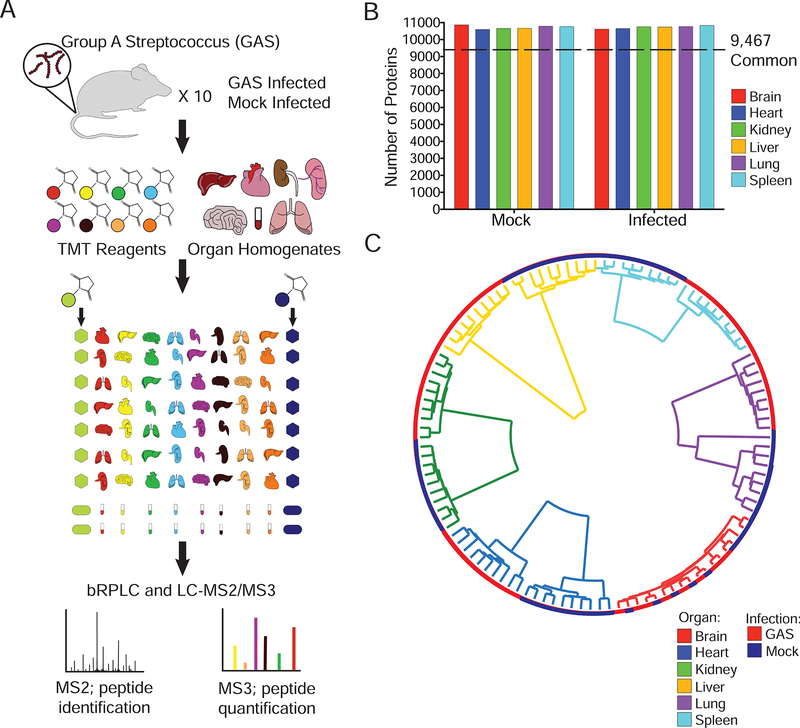
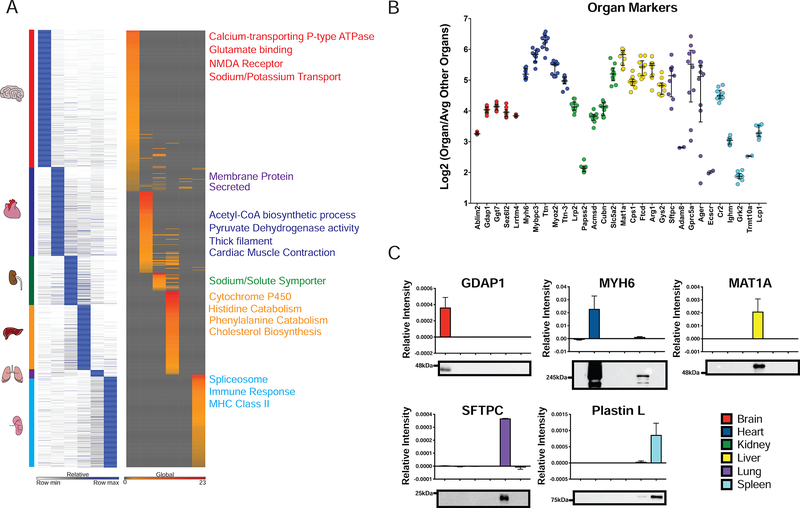
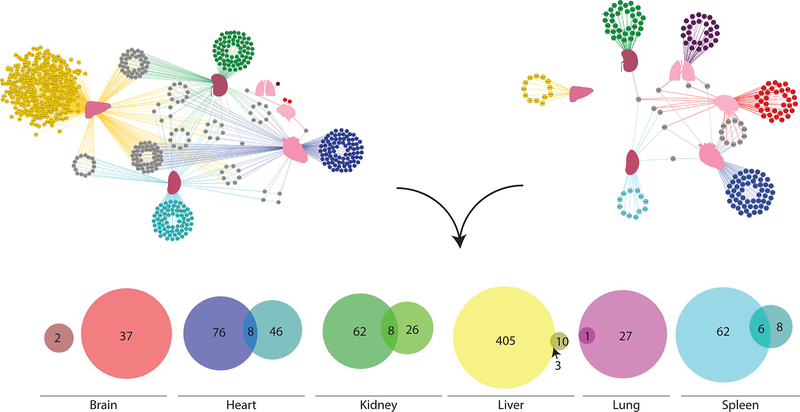
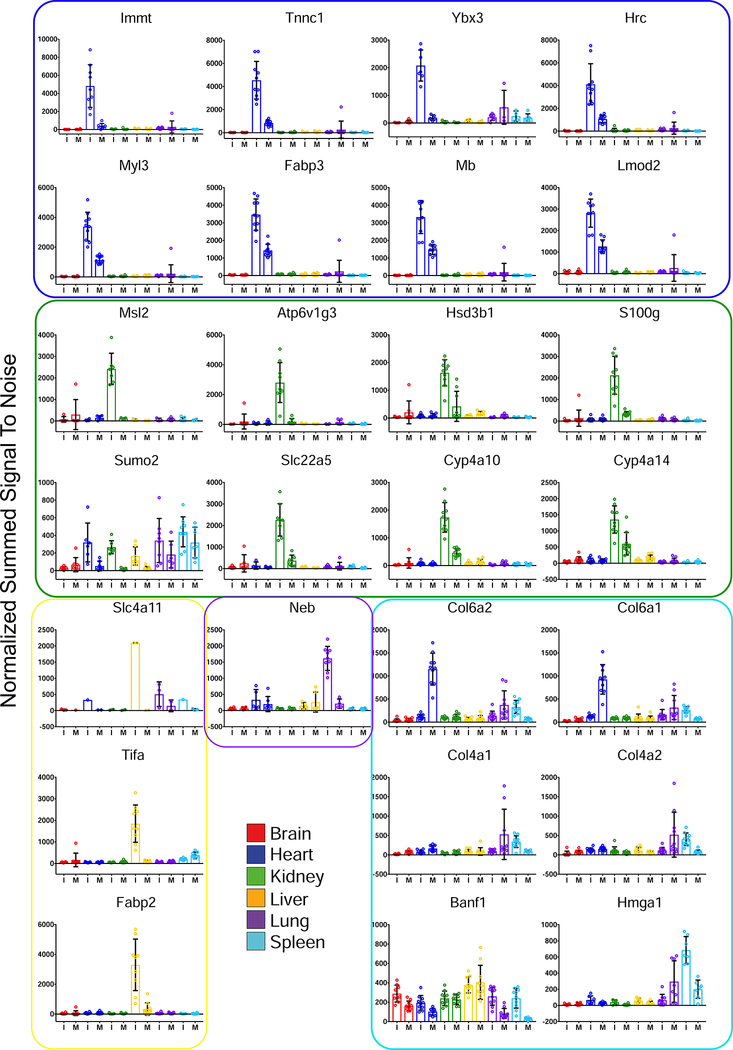
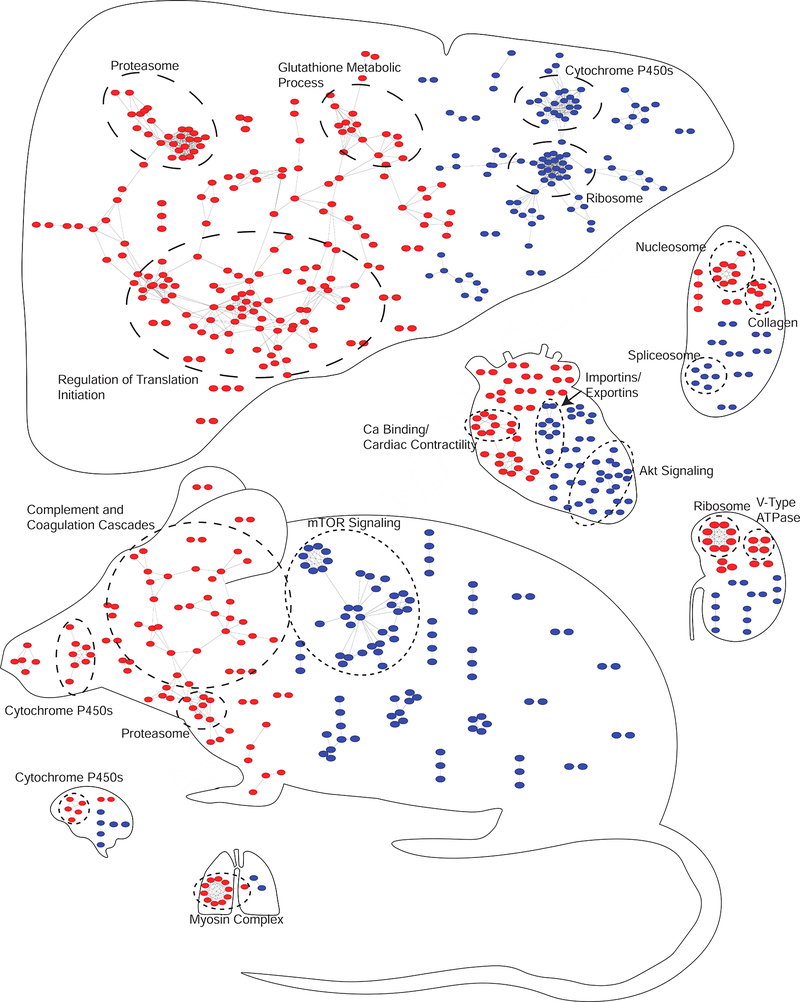
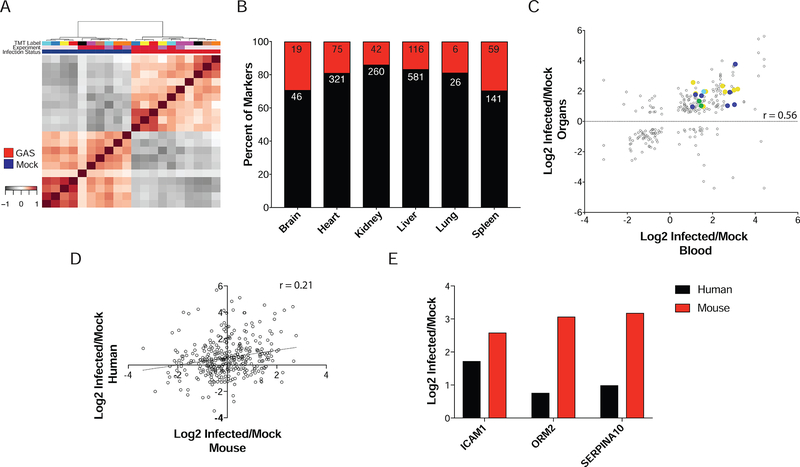
Group A Streptococcus (GAS) remains one of the top 10 deadliest human pathogens worldwide despite its sensitivity to penicillin. Although the most common GAS infection is pharyngitis (strep throat), it also causes life-threatening systemic infections. A series of complex networks between host and pathogen drive invasive infections, which have not been comprehensively mapped. Attempting to map these interactions, we examined organ-level protein dynamics using a mouse model of systemic GAS infection. We quantified over 11,000 proteins, defining organ-specific markers for all analyzed tissues. From this analysis, an atlas of dynamically regulated proteins and pathways was constructed. Through statistical methods, we narrowed organ-specific markers of infection to 34 from the defined atlas. We show these markers are trackable in blood of infected mice, and a subset has been observed in plasma samples from GAS-infected clinical patients. This proteomics-based strategy provides insight into host defense responses, establishes potentially useful targets for therapeutic intervention, and presents biomarkers for determining affected organs during bacterial infection.
Keywords: Orbitrap; S. pyogenes; Tandem Mass Tag; group A Streptococcus; multiplexed proteomics; systemic infection.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests
All authors declare no competing interests.
Figures
Comment in
-
A Host Proteome Atlas of Streptococcus pyogenes Infection.Cell Syst. 2018 May 23;6(5):536-538. doi: 10.1016/j.cels.2018.05.003. Cell Syst. 2018. PMID: 29792824
References
-
- AMMANN P, FEHR T, MINDER EI, GUNTER C & BERTEL O (2001). Elevation of troponin I in sepsis and septic shock. Intensive Care Med, 27, 965–9. - PubMed
-
- ASHBAUGH CD, MOSER TJ, SHEARER MH, WHITE GL, KENNEDY RC & WESSELS MR (2000). Bacterial determinants of persistent throat colonization and the associated immune response in a primate model of human group A streptococcal pharyngeal infection. Cell Microbiol, 2, 283–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
