

Case Reports
doi: 10.1016/j.jcmg.2018.04.005.
Epub 2018 May 16.
Predicting Left Ventricular Outflow Tract Obstruction Despite Anterior Mitral Leaflet Resection: The "Skirt NeoLVOT"
Affiliations
- PMID: 29778867
- PMCID: PMC6531676
- DOI: 10.1016/j.jcmg.2018.04.005
Item in Clipboard
Case Reports
Predicting Left Ventricular Outflow Tract Obstruction Despite Anterior Mitral Leaflet Resection: The "Skirt NeoLVOT"
JACC Cardiovasc Imaging.
2018 Sep.
No abstract available
Keywords: CT; complications; left ventricular outflow tract obstruction; mitral annular calcification; neo-LVOT; planning; transcatheter mitral valve replacement; transcoronary alcohol septal ablation; valve-in-MAC; valve-in-ring.
Figures
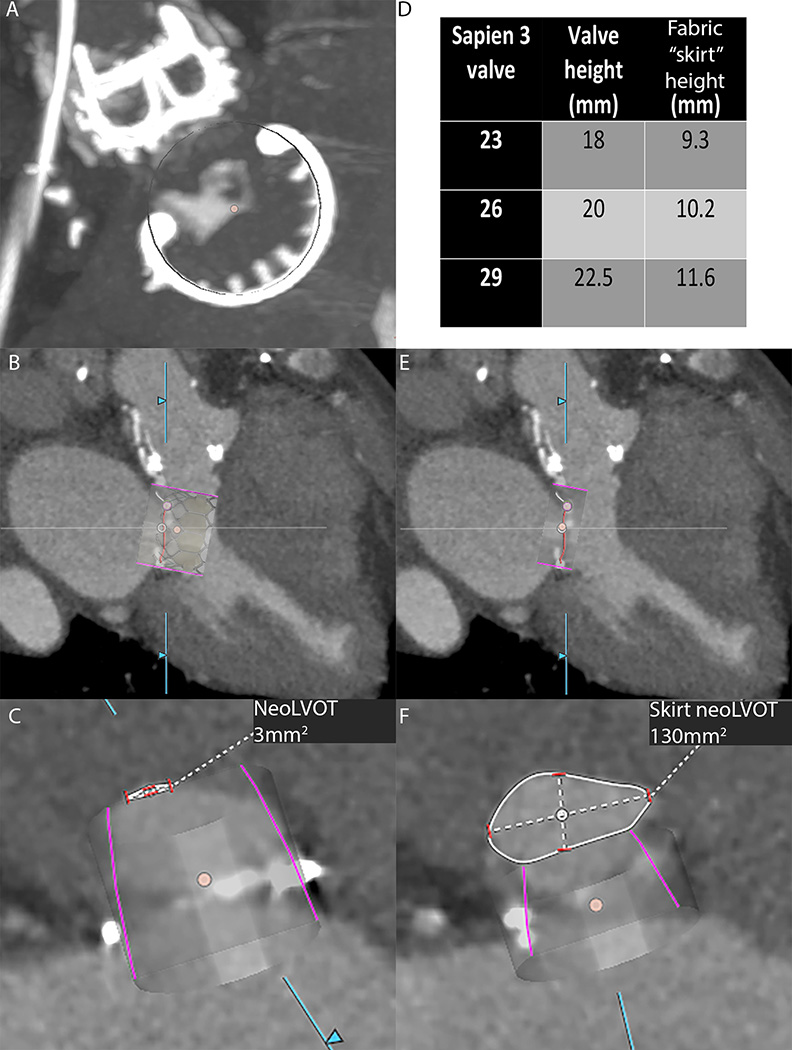
A 49-year-old woman with previous surgical aortic valve replacement and mitral
ring annuloplasty suffered severe mixed mitral valve disease and was prepared
for trans-septal TMVR. A) CT analysis suggests low risk of embolization and
paravalvular leak with a 26 Sapien3 valve. B) The three-chamber view
demonstrates risk factors for LVOT obstruction: a small ventricle, prominent
septal bulge, and acute aorto-mitral angulation. Using 3mensio software (Pie
Medical, Netherlands), a CT-simulated 26 Sapien3 valve is implanted at the
predicted orientation and depth. C) The orthogonal LVOT short-axis view shows a
predicted neoLVOT of 3mm2. To predict the LVOT after TMVR with
anterior leaflet resection, the “skirt” neoLVOT is calculated with
only the atrial skirt of the valve simulated (E), with height of 10mm as in
table (D). F) Her predicted “skirt neoLVOT” was 130mm2,
which predicts severe LVOT obstruction despite complete anterior mitral leaflet
resection.

The patient underwent LAMPOON TMVR. A) The fluoroscopy image shows two
transfemoral catheters with exposed guidewire kink (black arrow) at the center
and base of the anterior mitral leaflet. This guidewire is electrified while
applying tension to both catheters to lacerate the anterior leaflet down the
centerline. A deflectable sheath is positioned across the septum ready to
deliver the TMVR equipment, a pacing wire is at the right ventricular apex, and
a prior bioprosthetic aortic valve is present. B) The transesophageal
echocardiogram after LAMPOON laceration shows the split anterior mitral leaflet
(two white arrows). LA= Left atrium; LV = Left ventricle; Ao = Aorta

A) Transesophageal echocardiogram after TMVR demonstrates severe LVOT
obstruction. The skirt-covered valve cells (red double-headed arrow) span the
LVOT and the uncovered cells (black double-headed arrow) are against the septum
(white arrow heads). There is a narrow high velocity jet between the septum and
valve with a pressure drop of 114mmHg. B) Emergency transcoronary alcohol septal
ablation was performed with a balloon (arrow) occluding the first septal artery.
C) Transthoracic echocardiogram after emergency transcoronary alcohol septal
ablation demonstrates thinning of the septum and increased distance to the
transcatheter valve. D) Doppler flow is now seen through the open cells. E) On
post-procedure CT her neoLVOT measures 69mm2. The post-procedure
“skirt neoLVOT” area is 165mm2, which likely resembles
the physiological LV OT following LAMPOON as blood flows through the uncovered
cells, and final LVOT gradient is 20mmHg. LA= Left atrium; LV = Left ventricle;
Ao = Aorta

A) A 77-year-old woman with previous transcatheter aortic valve replacement and
severe mitral annular calcification and stenosis was planned to undergo
trans-septal TMVR. A 29mm Sapien3 is simulated at a 70:30 ventricular depth, which
would provide satisfactory seal and anchoring in this saddle-shaped annulus. B)
The predicted neoLVOT from the orthogonal plane is 0mm2. The overlap
between implanted valve and septum is 75mm2. C+D) The predicted
“skirt neoLVOT” for the patient is 137mm2 using a
CT-simulated valve height of 12mm and diameter of 29mm. This predicts severe
LVOT obstruction despite complete anterior leaflet resection.

A) Post-procedure CT reconstruction shows significant covered cell (small
diamonds/red doubleheaded arrows) protrusion into the LVOT. Her initial LVOT
gradient was 69mmHg. She underwent emergency transcoronary alcohol septal
ablation causing some thinning and akinesis of the septum, seen on CT, which
reduced her LVOT gradient to 41mmHg. B) Her post-implant neoLVOT was
0mm2, even after alcohol septal ablation, suggesting certain
death had LAMPOON not been performed. C) Her “skirt neoLVOT”,
which is likely to be her physiological LVOT after anterior leaflet
modification, is 150mm2.

A 76-year-old woman with severe mitral annular calcification and mitral stenosis
was planned for LAMPOON-TMVR with a 29mm Sapien3 valve (E). A) Trans-septal valve
positioning was predicted to be difficult because the small ventricle adversely
orienting the valve during balloon inflation (large arrow), risking anterior
miss and posterior paravalvular leak (small arrows). Controlling depth and
co-axial alignment may have been easier with trans-apical valve delivery, but
with increased morbidity. B-D) The neoLVOT was 0mm2 and skirt neoLVOT
(performed in retrospect) 55mm2. F) The valve tilted during
deployment, landing ventricular on the anterior side. The initial LVOT gradient
was 100mmHg, reducing to 50mmHg following emergency alcohol septal ablation. She
developed complete heart block and died post-op day 3. Necropsy shows the
anterior leaflet lacerated (yellow dashed lines) and parted to the side because
of LAMPOON. A significant portion of the LVOT was obstructed by the covered
cells of the valve.
References
-
- Blanke P, Naoum C, Dvir D et al. Predicting LVOT Obstruction in Transcatheter Mitral Valve Implantation: Concept of the Neo-LVOT. JACC Cardiovasc Imaging 2016:10.1016/j.jcmg.2016.01.005. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
