

Molecular genetics and metabolism, special edition: Diagnosis, diagnosis and prognosis of Mucopolysaccharidosis IVA
- PMID: 29779902
- PMCID: PMC6175643
- DOI: 10.1016/j.ymgme.2018.05.004
Molecular genetics and metabolism, special edition: Diagnosis, diagnosis and prognosis of Mucopolysaccharidosis IVA
Abstract
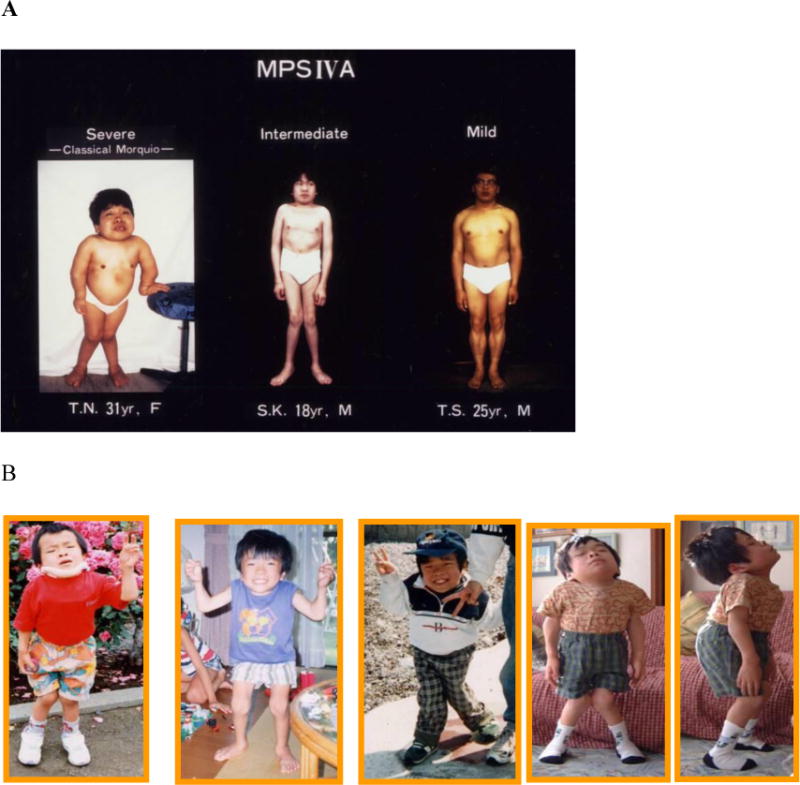
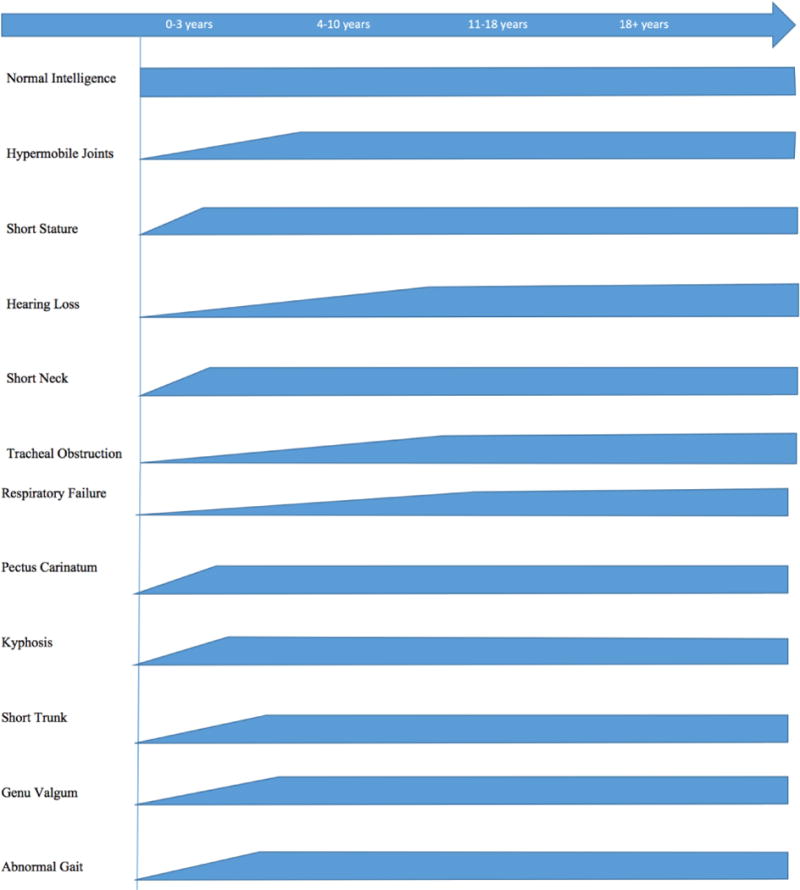
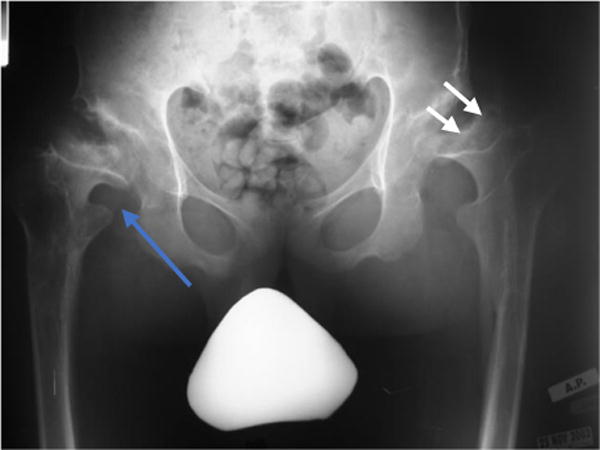
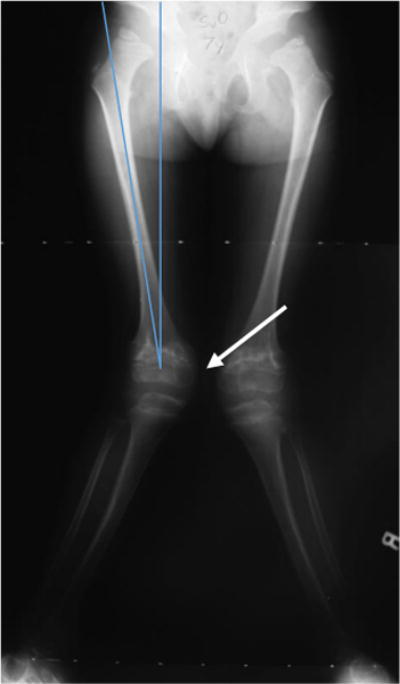
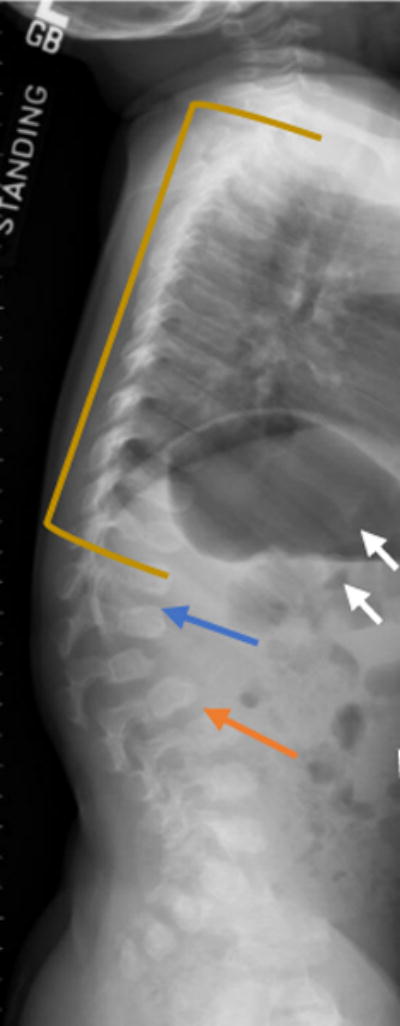
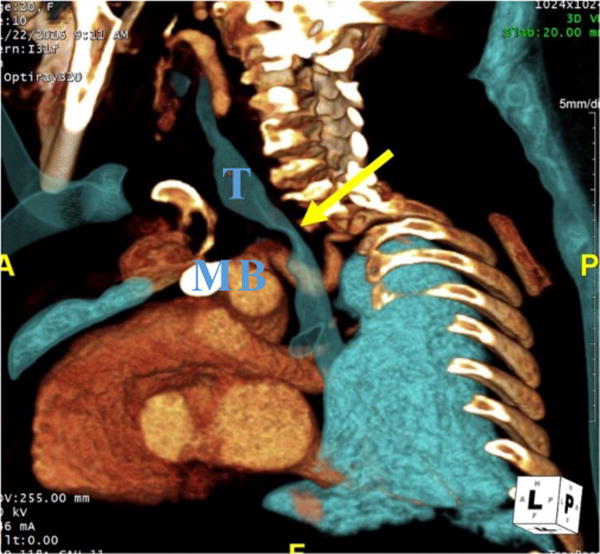
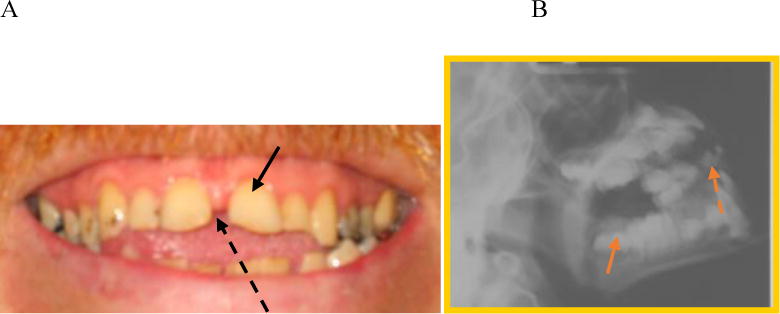
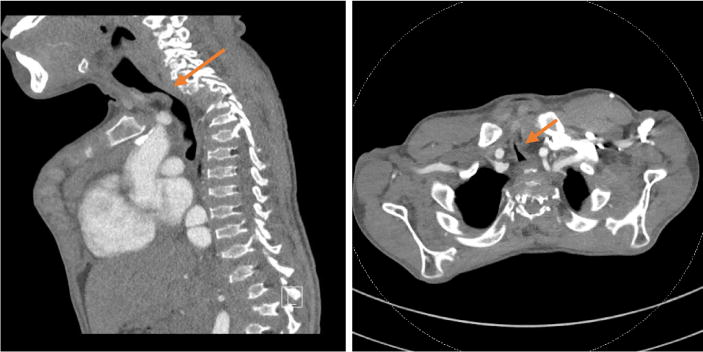
Mucopolysaccharidosis IVA (MPS IVA, Morquio A syndrome) is an autosomal recessive disorder caused by the deficiency of N-acetylgalactosamine-6-sulfate sulfatase. Deficiency of this enzyme leads to the accumulation of specific glycosaminoglycans (GAGs), chondroitin-6-sulfate (C6S) and keratan sulfate (KS), which are mainly synthesized in the cartilage. Therefore, the substrates are stored primarily in the cartilage and its extracellular matrix (ECM), leading to a direct impact on bone development and successive systemic skeletal spondylepiphyseal dysplasia. The skeletal-related symptoms for MPS IVA include short stature with short neck and trunk, odontoid hypoplasia, spinal cord compression, tracheal obstruction, obstructive airway, pectus carinatum, restrictive lung, kyphoscoliosis, platyspondyly, coxa valga, genu valgum, waddling gait, and laxity of joints. The degree of imbalance of growth in bone and other organs and tissues largely contributes to unique skeletal dysplasia and clinical severity. Diagnosis of MPS IVA needs clinical, radiographic, and laboratory testing to make a complete conclusion. To diagnose MPS IVA, total urinary GAG analysis which has been used is problematic since the values overlap with those in age-matched controls. Currently, urinary and blood KS and C6S, the enzyme activity of GALNS, and GALNS molecular analysis are used for diagnosis and prognosis of clinical phenotype in MPS IVA. MPS IVA can be diagnosed with unique characters although this disorder relates closely to other disorders in some characteristics. In this review article, we comprehensively describe clinical, radiographic, biochemical, and molecular diagnosis and clinical assessment tests for MPS IVA. We also compare MPS IVA to other closely related disorders to differentiate MPS IVA. Overall, imbalance of growth in MPS IVA patients underlies unique skeletal manifestations leading to a critical indicator for diagnosis.
Keywords: Chondroitin-6-sulfate; Keratan sulfate; Mucopolysaccharidosis IVA; N-acetylgalactosamine-6-sulfate; Spondyloepiphyseal dysplasia.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
All the authors contributed to the Review Article and had no conflict of interest with any other party. Hira Peracha, Kazuki Sawamoto, Lauren Averill, Heidi Kecskemethy, Mary Theroux, Mihir Thacker, Kyoko Nagao, Christian Pizarro, William Mackenzie, Hironori Kobayashi, Seiji Yamaguchi, Yasuyuki Suzuki, Kenji Orii, Tadao Orii, Toshiyuki Fukao, Shunji Tomatsu declare that they have no conflict of interests.
Figures




References
-
- Gentili C, Cancedda R. Cartilage and bone extracellular matrix. Curr Pharm Des. 2009;15:1334–48. http://www.ncbi.nlm.nih.gov/pubmed/19355972 (accessed October 28, 2017) - PubMed
-
- Morquio L. Sur une forme de dystrophie osseuse familiale. Bull Soc Pediatr Paris. 1929;27:145–52.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
