

Managing portal hypertension in patients with liver cirrhosis
- PMID: 29780579
- PMCID: PMC5934688
- DOI: 10.12688/f1000research.13943.1
Managing portal hypertension in patients with liver cirrhosis
Abstract
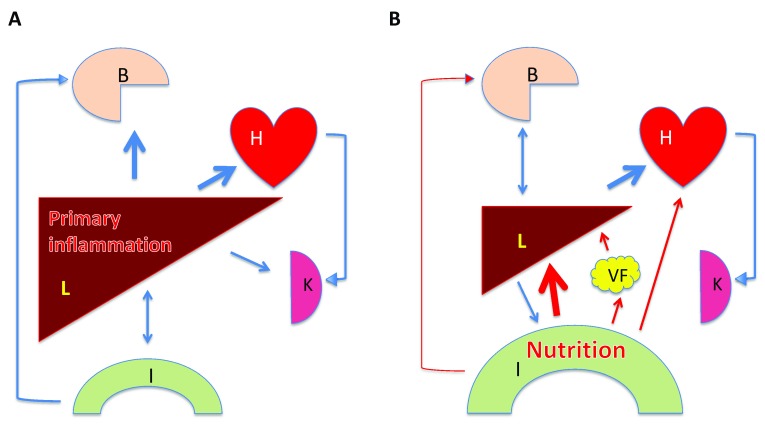
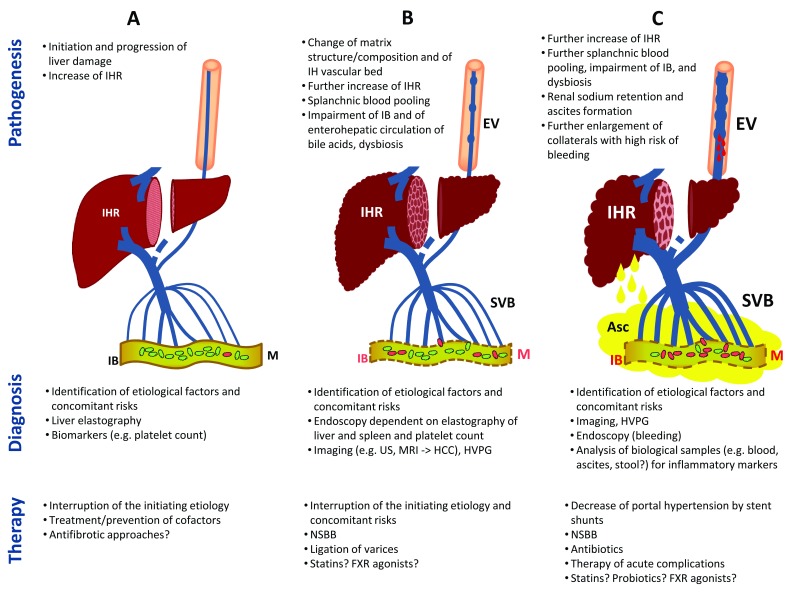
Portal hypertension is one cause and a part of a dynamic process triggered by chronic liver disease, mostly induced by alcohol or incorrect nutrition and less often by viral infections and autoimmune or genetic disease. Adequate staging - continuously modified by current knowledge - should guide the prevention and treatment of portal hypertension with defined endpoints. The main goals are interruption of etiology and prevention of complications followed, if necessary, by treatment of these. For the past few decades, shunts, mostly as intrahepatic stent bypass between portal and hepatic vein branches, have played an important role in the prevention of recurrent bleeding and ascites formation, although their impact on survival remains ambiguous. Systemic drugs, such as non-selective beta-blockers, statins, or antibiotics, reduce portal hypertension by decreasing intrahepatic resistance or portal tributary blood flow or by blunting inflammatory stimuli inside and outside the liver. Here, the interactions among the gut, liver, and brain are increasingly examined for new therapeutic options. There is no general panacea. The interruption of initiating factors is key. If not possible or if not possible in a timely manner, combined approaches should receive more attention before considering liver transplantation.
Keywords: chronic liver disease; liver cirrhosis; portal hypertension.
Conflict of interest statement
No competing interests were disclosed.No competing interests were disclosed.No competing interests were disclosed.
Figures
References
-
- Fallon MB, Abrams GA: Hepatopulmonary syndrome. Curr Gastroenterol Rep. 2000;2(1):40–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous