

Confocal Microscopy in Skin Cancer
- PMID: 29780659
- PMCID: PMC5956038
- DOI: 10.1007/s13671-018-0218-9
Confocal Microscopy in Skin Cancer
Abstract
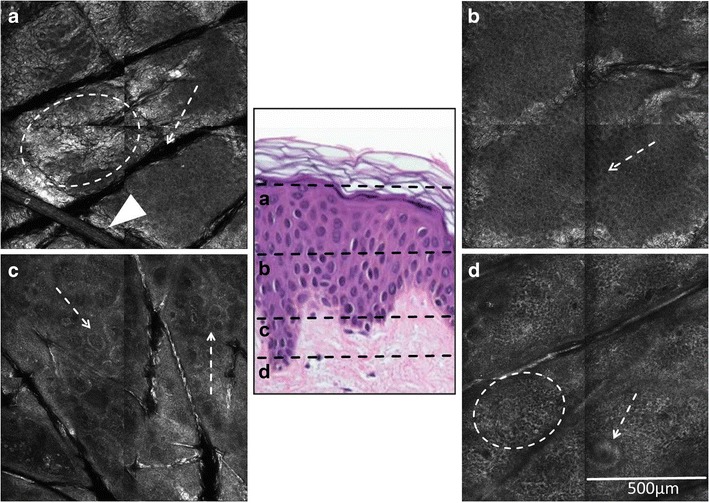
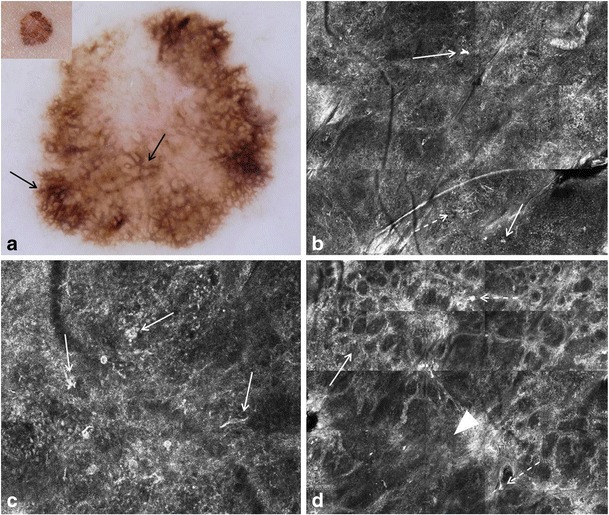
Purpose of review: Reflectance confocal microscopy (RCM) enables imaging of skin lesions at cellular level resolution at the bedside (in vivo) or in freshly excised tissue (ex vivo). This article provides an overview of strengths and limitations of non-invasive RCM in skin cancer diagnosis.
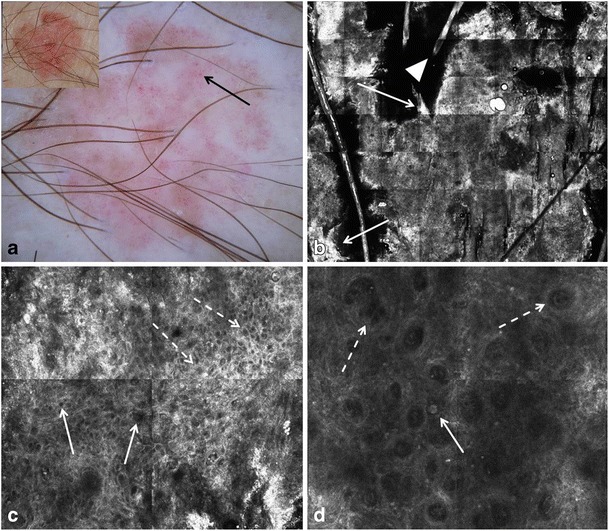
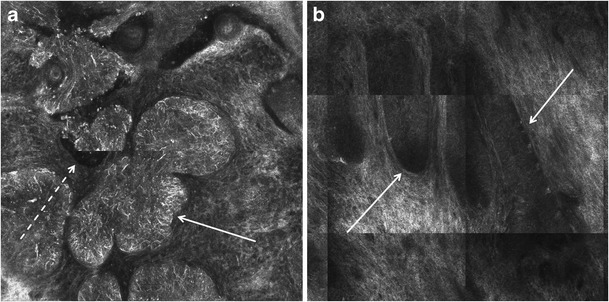
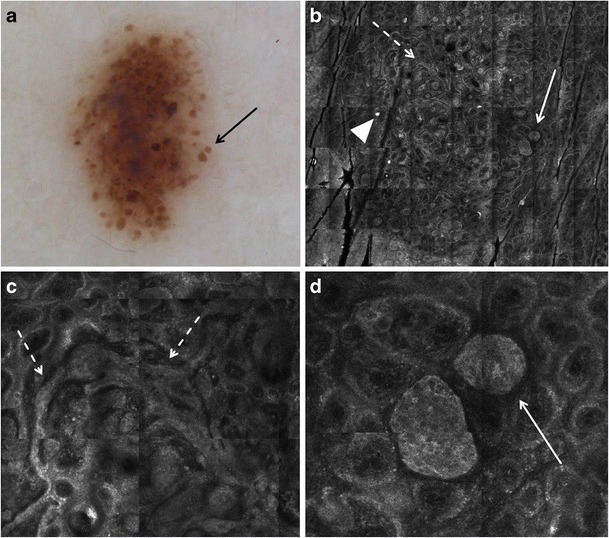
Recent findings: RCM features of common melanocytic and non-melanocytic skin neoplasms such as melanoma, actinic keratosis/squamous cell carcinoma, basal cell carcinoma, and nevi have been well defined and show good correlation with dermoscopic and histopathologic findings. Due to its technical properties, RCM is especially suitable for the examination of flat skin lesions.
Summary: In vivo RCM has been shown to increase the accuracy of non-invasive diagnosis of common skin neoplasms and is a valuable adjunct to dermoscopy, particularly in cosmetically and functionally sensitive areas such as the face or the genital area.
Keywords: Basal cell carcinoma; Dermoscopy; Facial macules; Histopathology; Lentigo maligna; Melanoma; Nevi; Non-melanoma skin cancer; Reflectance confocal microscopy; Skin tumors.
Conflict of interest statement
Compliance with Ethical StandardsThe authors declare that they have no conflict of interest.This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures



References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials