

Total aortic repair for acute type A aortic dissection: a new paradigm
- PMID: 29780725
- PMCID: PMC5945912
- DOI: 10.21037/jovs.2018.04.04
Total aortic repair for acute type A aortic dissection: a new paradigm
Abstract
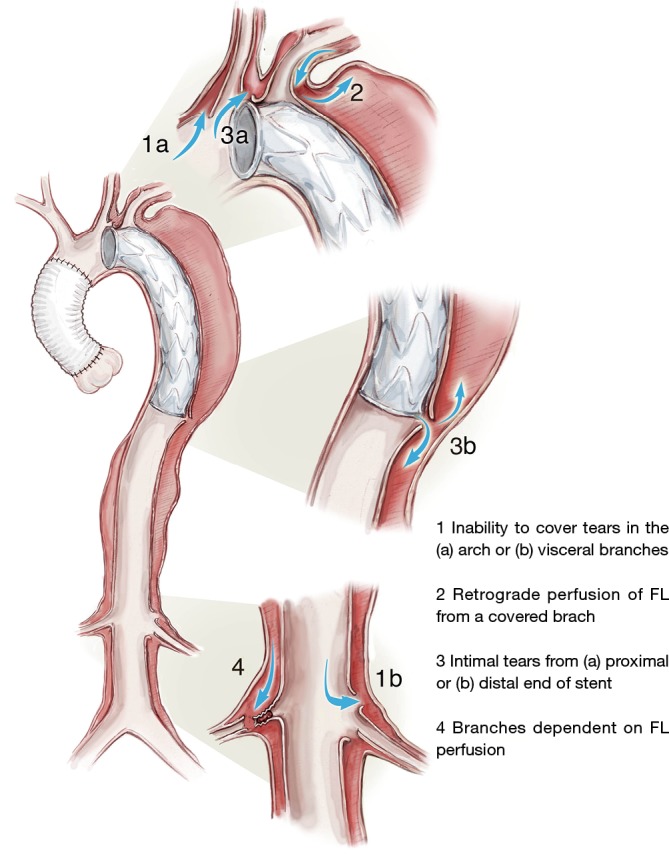
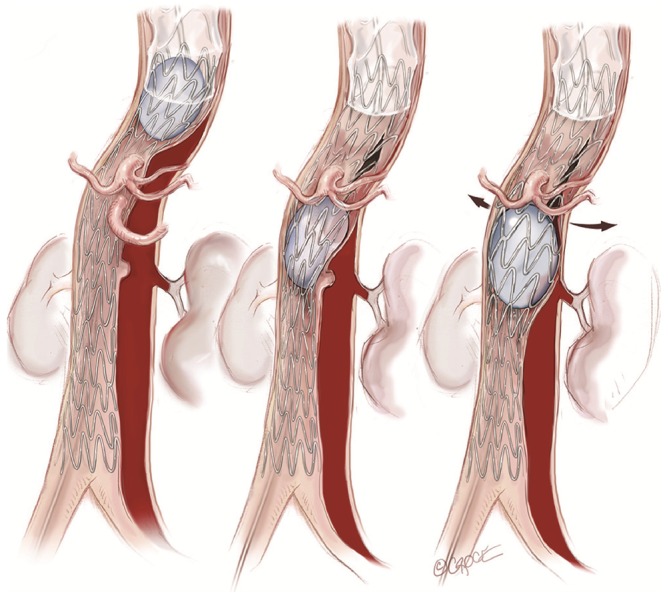
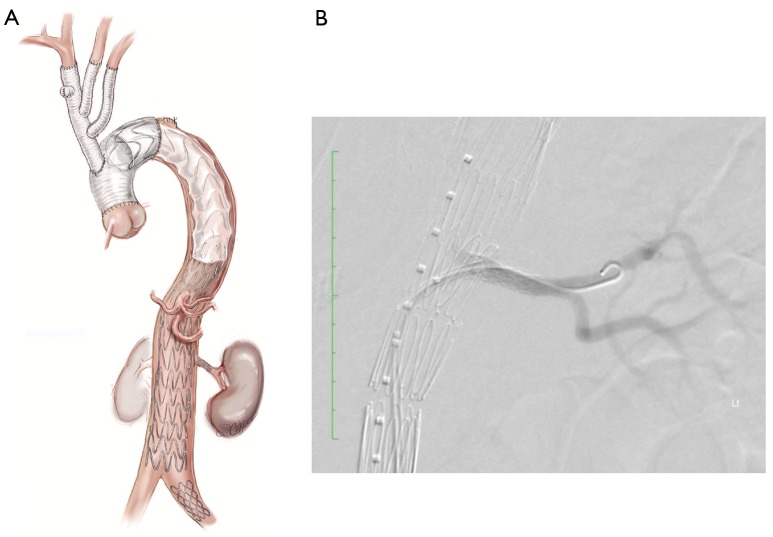
The currently accepted guidelines of open surgical repair for acute type A aortic dissection (ATAAD) include the resection of the primary entry tear, replacement of the ascending aorta and "hemi-arch" with an open distal anastomosis, and aortic valve resuspension and some form of obliteration of the aortic root false lumen. The principal aim being protection against aortic rupture, aortic regurgitation, and coronary ischemia and restoration of antegrade preferential true lumen perfusion. Proponents argue that this operation is tailored to be in the armamentarium of most cardiac surgeons and deliver the lowest early operative risk, while leaving the infrequent long-term sequelae to be dealt with electively by experienced aortic centres. While a superficially compelling argument, the actual outcomes suggest that it falls significantly short of achieving its noble goals on both acute and chronic counts. This led us to develop a seemingly more radical but in practise safe paradigm, which aims to achieve total aortic healing in the acute phase.
Keywords: Aorta; dissection; endovascular stenting.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
A new paradigm in the management of acute type A aortic dissection: Total aortic repair.J Thorac Cardiovasc Surg. 2019 Jan;157(1):3-11. doi: 10.1016/j.jtcvs.2018.08.118. Epub 2018 Oct 13. J Thorac Cardiovasc Surg. 2019. PMID: 30557944
-
Total aortic repair: the new paradigm in the treatment of acute type A aortic dissection.Ann Cardiothorac Surg. 2016 May;5(3):216-21. doi: 10.21037/acs.2016.05.02. Ann Cardiothorac Surg. 2016. PMID: 27386409 Free PMC article.
-
Surgical management of acute type A aortic dissection: branch-first arch replacement with total aortic repair.Ann Cardiothorac Surg. 2016 May;5(3):236-44. doi: 10.21037/acs.2016.05.11. Ann Cardiothorac Surg. 2016. PMID: 27386413 Free PMC article. Review.
-
Descending endografts for type A dissections: con.Ann Cardiothorac Surg. 2016 May;5(3):227-32. doi: 10.21037/acs.2016.04.03. Ann Cardiothorac Surg. 2016. PMID: 27386411 Free PMC article.
-
Spontaneous retrograde dissection of ascending aorta from descending thoracic aorta--a case review.Perfusion. 2011 May;26(3):215-22. doi: 10.1177/0267659110395804. Epub 2011 Jan 19. Perfusion. 2011. PMID: 21247986 Review.
Cited by
-
Brachiocephalic Artery Dissection Following Type A Aortic Dissection Repair.Cureus. 2023 Dec 31;15(12):e51379. doi: 10.7759/cureus.51379. eCollection 2023 Dec. Cureus. 2023. PMID: 38292995 Free PMC article.
-
Evaluation of Different Cannulation Strategies for Aortic Arch Surgery Using a Cardiovascular Numerical Simulator.Bioengineering (Basel). 2023 Jan 3;10(1):60. doi: 10.3390/bioengineering10010060. Bioengineering (Basel). 2023. PMID: 36671632 Free PMC article.
-
Quantifying the learning curve of emergent total arch replacement in acute type A aortic dissection.J Thorac Dis. 2020 Aug;12(8):4070-4081. doi: 10.21037/jtd-20-912. J Thorac Dis. 2020. PMID: 32944318 Free PMC article.
-
The aortic arch management for type A aortic dissection: aggressive but experienced.J Thorac Dis. 2020 Jun;12(6):3429-3432. doi: 10.21037/jtd.2020.01.58. J Thorac Dis. 2020. PMID: 32642271 Free PMC article. No abstract available.
-
Alternative Approach for Cerebral Protection during Complex Aortic Arch and Redo Surgery.J Cardiovasc Dev Dis. 2021 Jul 27;8(8):86. doi: 10.3390/jcdd8080086. J Cardiovasc Dev Dis. 2021. PMID: 34436228 Free PMC article.
References
-
- Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010;121:e266-369. 10.1161/CIR.0b013e3181d4739e - DOI - PubMed
-
- Erbel R, Aboyans V, Boileau C, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J 2014;35:2873-926. 10.1093/eurheartj/ehu281 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources