

Procalcitonin-Guided Use of Antibiotics for Lower Respiratory Tract Infection
- PMID: 29781385
- PMCID: PMC6197800
- DOI: 10.1056/NEJMoa1802670
Procalcitonin-Guided Use of Antibiotics for Lower Respiratory Tract Infection
Abstract
Background: The effect of procalcitonin-guided use of antibiotics on treatment for suspected lower respiratory tract infection is unclear.
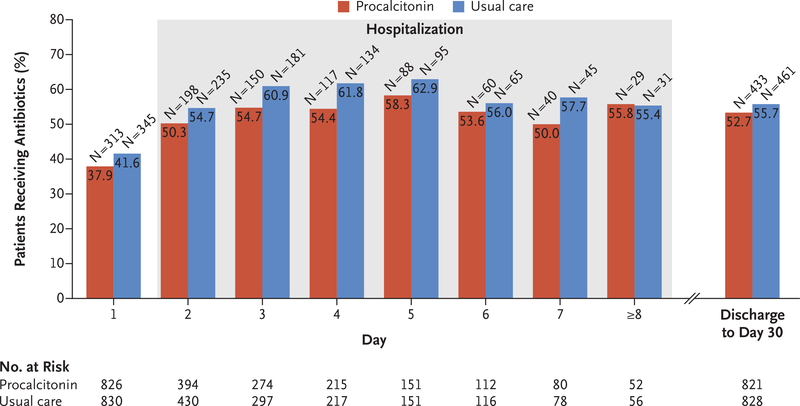
Methods: In 14 U.S. hospitals with high adherence to quality measures for the treatment of pneumonia, we provided guidance for clinicians about national clinical practice recommendations for the treatment of lower respiratory tract infections and the interpretation of procalcitonin assays. We then randomly assigned patients who presented to the emergency department with a suspected lower respiratory tract infection and for whom the treating physician was uncertain whether antibiotic therapy was indicated to one of two groups: the procalcitonin group, in which the treating clinicians were provided with real-time initial (and serial, if the patient was hospitalized) procalcitonin assay results and an antibiotic use guideline with graded recommendations based on four tiers of procalcitonin levels, or the usual-care group. We hypothesized that within 30 days after enrollment the total antibiotic-days would be lower - and the percentage of patients with adverse outcomes would not be more than 4.5 percentage points higher - in the procalcitonin group than in the usual-care group.
Results: A total of 1656 patients were included in the final analysis cohort (826 randomly assigned to the procalcitonin group and 830 to the usual-care group), of whom 782 (47.2%) were hospitalized and 984 (59.4%) received antibiotics within 30 days. The treating clinician received procalcitonin assay results for 792 of 826 patients (95.9%) in the procalcitonin group (median time from sample collection to assay result, 77 minutes) and for 18 of 830 patients (2.2%) in the usual-care group. In both groups, the procalcitonin-level tier was associated with the decision to prescribe antibiotics in the emergency department. There was no significant difference between the procalcitonin group and the usual-care group in antibiotic-days (mean, 4.2 and 4.3 days, respectively; difference, -0.05 day; 95% confidence interval [CI], -0.6 to 0.5; P=0.87) or the proportion of patients with adverse outcomes (11.7% [96 patients] and 13.1% [109 patients]; difference, -1.5 percentage points; 95% CI, -4.6 to 1.7; P<0.001 for noninferiority) within 30 days.
Conclusions: The provision of procalcitonin assay results, along with instructions on their interpretation, to emergency department and hospital-based clinicians did not result in less use of antibiotics than did usual care among patients with suspected lower respiratory tract infection. (Funded by the National Institute of General Medical Sciences; ProACT ClinicalTrials.gov number, NCT02130986 .).
Figures


Comment in
-
Procalcitonin-guided antibiotic prescribing did not reduce antibiotic use in suspected LRTI in the ED.Ann Intern Med. 2018 Oct 16;169(8):JC39. doi: 10.7326/ACPJC-2018-169-8-039. Ann Intern Med. 2018. PMID: 30326083 No abstract available.
-
Procalcitonin-Guided Antibiotic Use.N Engl J Med. 2018 Nov 15;379(20):1971-2. doi: 10.1056/NEJMc1811150. N Engl J Med. 2018. PMID: 30439285 Free PMC article. No abstract available.
-
Procalcitonin-Guided Antibiotic Use.N Engl J Med. 2018 Nov 15;379(20):1972. doi: 10.1056/NEJMc1811150. N Engl J Med. 2018. PMID: 30439286 No abstract available.
-
Procalcitonin-Guided Antibiotic Use.N Engl J Med. 2018 Nov 15;379(20):1972-3. doi: 10.1056/NEJMc1811150. N Engl J Med. 2018. PMID: 30439593 No abstract available.
References
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 2016; 315: 1864–73. - PubMed
-
- Nathan C, Cars O. Antibiotic resistance — problems, progress, and prospects. N Engl J Med 2014; 371: 1761–3. - PubMed
-
- Linder JA. Antibiotic prescribing for acute respiratory infections — success that’s way off the mark: comment on “A cluster randomized trial of decision support strategies for reducing antibiotic use in acute bronchitis.” JAMA Intern Med 2013;173: 273–5. - PubMed
-
- Antibiotic use in the United States, 2017: progress and opportunities. Atlanta: Centers for Disease Control and Prevention, 2017. (https://www.cdc.gov/antibiotic-use/stewardship-report/hospital.html).
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical