

Cognitive Burden of Common Non-antiretroviral Medications in HIV-Infected Women
- PMID: 29781879
- PMCID: PMC6092212
- DOI: 10.1097/QAI.0000000000001755
Cognitive Burden of Common Non-antiretroviral Medications in HIV-Infected Women
Abstract
Objective: The aging HIV population has increased comorbidity burden and consequently non-antiretroviral medication utilization. Many non-antiretroviral medications have known neurocognitive-adverse effects ("NC-AE medications"). We assessed the cognitive effects of NC-AE medications in HIV+ and HIV- women.
Methods: One thousand five hundred fifty-eight participants (1037 HIV+; mean age 46) from the Women's Interagency HIV Study completed a neuropsychological test battery between 2009 and 2011. The total number of NC-AE medications and subgroups (eg, anticholinergics) were calculated based on self-report. Generalized linear models for non-normal data were used to examine the cognitive burden of medications and factors that exacerbate these effects.
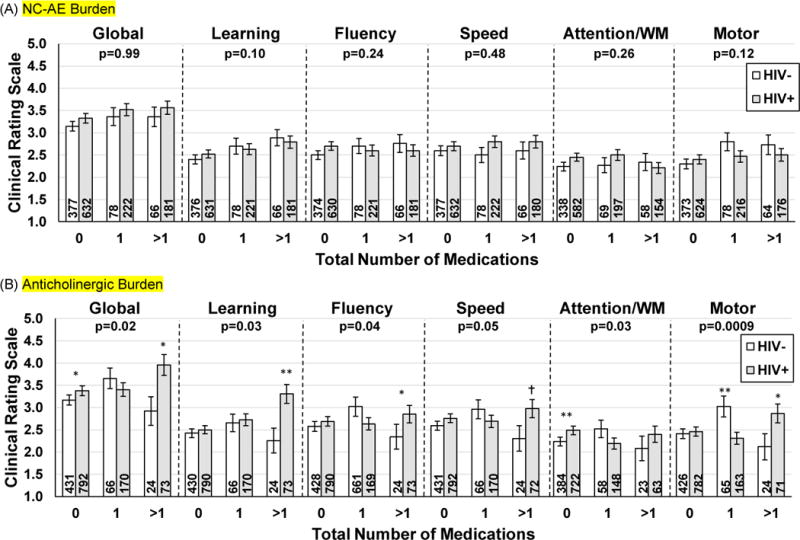
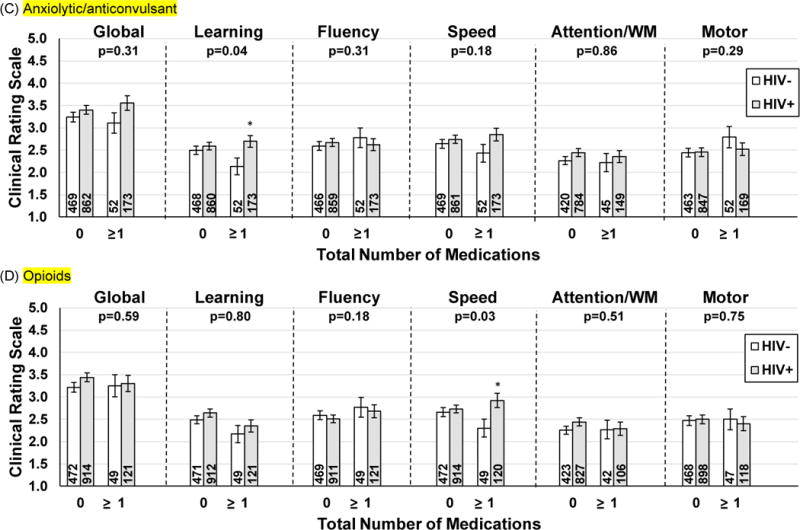
Results: HIV+ women reported taking more NC-AE medications vs. HIV- women (P < 0.05). NC-AE medication use altogether was not associated with cognitive performance. However, among NC-AE medication subgroups, anticholinergic-acting medications, but not opioids or anxiolytics/anticonvulsants, were negatively associated with performance. HIV status moderated the association between these NC-AE medication subgroups and performance (P's < 0.05). HIV-serostatus differences (HIV- < HIV+) in global, learning, fluency, and motor function were greatest among women taking >1 anticholinergic medications. HIV-serostatus differences in performance on learning and psychomotor speed were also greatest among women taking 1 or more anxiolytics/anticonvulsants and 1 or more opioids, respectively.
Conclusions: HIV+ women have increased cognitive vulnerabilities to anticholinergic, anxiolytic/anticonvulsant, and opioid medications. Potential synergy between these medications and HIV may explain some HIV-related cognitive impairments. It may be important clinically to consider these specific types of medications as a contributor to impaired cognitive performance in HIV+ women and assess the cost/benefit of treatment dosage for underlying conditions.
Conflict of interest statement
Figures
Similar articles
-
Use of Nonantiretroviral Medications That May Impact Neurocognition: Patterns and Predictors in a Large, Long-Term HIV Cohort Study.J Acquir Immune Defic Syndr. 2018 Jun 1;78(2):202-208. doi: 10.1097/QAI.0000000000001658. J Acquir Immune Defic Syndr. 2018. PMID: 29762344 Free PMC article.
-
Long-term efavirenz use is associated with worse neurocognitive functioning in HIV-infected patients.J Neurovirol. 2016 Apr;22(2):170-8. doi: 10.1007/s13365-015-0382-7. Epub 2015 Sep 25. J Neurovirol. 2016. PMID: 26407716 Free PMC article.
-
Impaired Cognition Predicts Falls Among Women With and Without HIV Infection.J Acquir Immune Defic Syndr. 2020 Mar 1;83(3):301-309. doi: 10.1097/QAI.0000000000002262. J Acquir Immune Defic Syndr. 2020. PMID: 31913989 Free PMC article.
-
Aging and Neurocognitive Functioning in HIV-Infected Women: a Review of the Literature Involving the Women's Interagency HIV Study.Curr HIV/AIDS Rep. 2016 Dec;13(6):399-411. doi: 10.1007/s11904-016-0340-x. Curr HIV/AIDS Rep. 2016. PMID: 27730446 Free PMC article. Review.
-
Risk factors for cognitive decline in persons with HIV.Curr Opin Infect Dis. 2025 Feb 1;38(1):37-43. doi: 10.1097/QCO.0000000000001080. Epub 2024 Dec 6. Curr Opin Infect Dis. 2025. PMID: 39641182 Free PMC article. Review.
Cited by
-
The Effects of Prescribed Medications on Depressive Symptoms and Neurocognitive Performance in People With HIV.Clin Infect Dis. 2025 Apr 30;80(4):871-880. doi: 10.1093/cid/ciae518. Clin Infect Dis. 2025. PMID: 39658021
-
Tablet-Based Cognitive Impairment Screening for Adults With HIV Seeking Clinical Care: Observational Study.JMIR Ment Health. 2021 Sep 9;8(9):e25660. doi: 10.2196/25660. JMIR Ment Health. 2021. PMID: 34499048 Free PMC article.
-
Predicting Neurobehavioral Outcomes in People with HIV.Res Sq [Preprint]. 2025 Mar 27:rs.3.rs-5618870. doi: 10.21203/rs.3.rs-5618870/v1. Res Sq. 2025. PMID: 40195986 Free PMC article. Preprint.
-
The association between benzodiazepine use and greater risk of neurocognitive impairment is moderated by medical burden in people with HIV.J Neurovirol. 2022 Jun;28(3):410-421. doi: 10.1007/s13365-022-01076-1. Epub 2022 Apr 7. J Neurovirol. 2022. PMID: 35389174 Free PMC article.
-
Special Topics in the Care of Older People with HIV.Curr Treat Options Infect Dis. 2019 Dec;11(4):388-400. doi: 10.1007/s40506-019-00204-6. Epub 2019 Nov 8. Curr Treat Options Infect Dis. 2019. PMID: 33343235 Free PMC article.
References
-
- HIV Among People Aged 50 and Over. Centers for Disease Control and Prevention; 2015.
-
- Grant I. Neurocognitive disturbances in HIV. Int Rev Psychiatry. 2008;20(1):33–47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI103397/AI/NIAID NIH HHS/United States
- U01 AI031834/AI/NIAID NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- U01 AI103401/AI/NIAID NIH HHS/United States
- U01 AI103408/AI/NIAID NIH HHS/United States
- K01 MH098798/MH/NIMH NIH HHS/United States
- U01 AI103390/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
