

Evaluation of idiopathic olfactory loss with chemosensory event-related potentials and magnetic resonance imaging
- PMID: 29782071
- PMCID: PMC6282607
- DOI: 10.1002/alr.22144
Evaluation of idiopathic olfactory loss with chemosensory event-related potentials and magnetic resonance imaging
Abstract
Background: Idiopathic olfactory loss (IOL) accounts for a sizable fraction of olfactory dysfunction, but very little is known about its etiology and electrophysiological changes in the olfactory pathway.
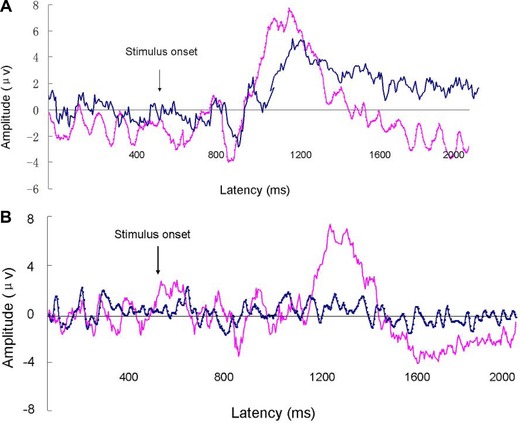
Methods: We analyzed the physiology of IOL using chemosensory event-related potentials (ERPs) (olfactory and trigeminal: oERP and tERP) and olfactory pathway magnetic resonance imaging (MRI) measured in adult patients with IOL and healthy controls. Subjective olfactory function was measured by Toyota and Takagi (T&T) olfactometry and Sniffin' Sticks (SS).
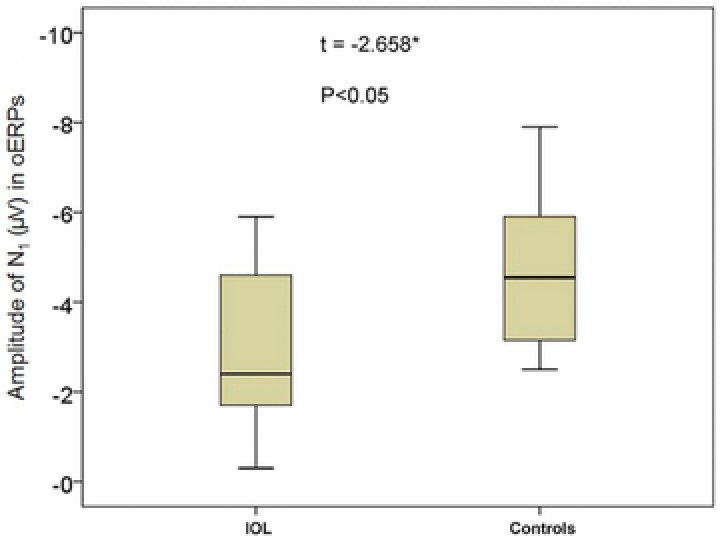
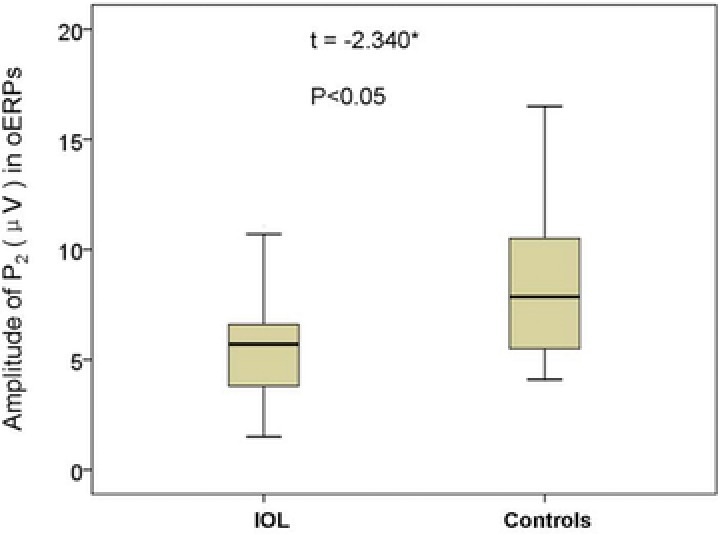
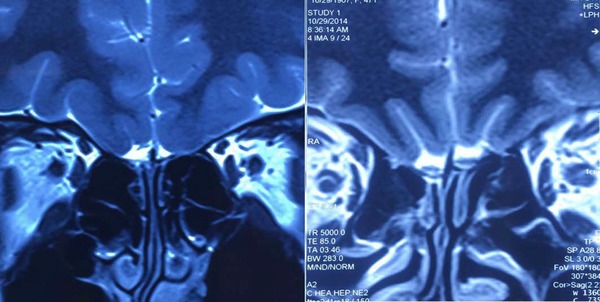
Results: Olfactory function was worse in patients with IOL compared to controls (T&T, p < 0.001; SS, p < 0.001). oERPs could be evoked in 17 IOL patients. Signals in these patients showed lower amplitude in the N1 and P2 waves than controls (p < 0.05 for both), but there were no difference in latency between the 2 groups (p > 0.05). tERP were detected in all patients and controls; there were no differences in latency and nor amplitude between the 2 groups (p > 0.05). The olfactory bulb (OB) volume was significantly smaller in the IOL group than controls (p < 0.001), but there was no difference in the olfactory sulcus depth between groups (p > 0.05). Better olfactory function was associated with increasing magnitude of N1 amplitude in oERPs (p < 0.05) and increasing OB volume (p < 0.05).
Conclusion: IOL patients show neurophysiologic deficits and some anatomic differences compared to healthy controls.
背景: 尽管特发性嗅觉下降 (IOL) 在嗅觉障碍人群中所占比例相当可观, 但是相关病因学机制及嗅觉通路相关电生理变化并不十分清楚。
方法: 通过对比成人IOL及健康人群的化学感受事件相关电位 (ERPs) 及嗅觉通路核磁共振成像 (MRI) 的差异, 我们分析IOL的生理机制。同时采用Toyota和Takagi (T&T) 嗅觉测定法及Sniffin'Sticks嗅觉心理物理测试 (SS) 对患者主观嗅功能进行评定。
结果: 与对照组相比, IOL患者嗅功能更差(T&T, p < 0.001; SS, p < 0.001)。17例IOL患者诱发出oERPs (嗅神经化学感受事件相关电位) , 这些患者N1、P2波振幅与对照组相比明显降低(p 均 < 0.05), 但两组间潜伏期无明显差异(p > 0.05)。所有患者及健康人群均能检测出tERP (三叉神经感受事件相关电位) ;两组间潜伏期、振幅变化无统计学差异(p > 0.05)。IOL组嗅球 (OB) 体积明显小于对照组(p < 0.001), 但组间嗅裂深度无统计学差异(p >0.05)。嗅觉功能与oERPs中N1振幅幅度、OB体积呈正相关(p 均< 0.05)。
结论: 与健康对照组相比, IOL患者呈现出部分神经生理学缺陷及解剖学异常。
Keywords: MRI; chemosensory event-related potentials; clinical features; idiopathic olfactory loss; olfactory function.
© 2018 The Authors. International Forum of Allergy & Rhinology published by Wiley Periodicals, Inc. on behalf of American Academy of Otolaryngic Allergy and American Rhinologic Society.
Figures
References
-
- Henkin RI, Levy LM, Fordyce A. Taste and smell function in chronic disease: a review of clinical and biochemical evaluations of taste and smell dysfunction in over 5000 patients at The Taste and Smell Clinic in Washington, DC. Am J Otolaryngol. 2013;34:477–489. - PubMed
-
- Damm M, Temmel A, Welge‐Lüssen A, et al. [Olfactory dysfunctions. Epidemiology and therapy in Germany, Austria and Switzerland]. HNO. 2004;52:112–120. - PubMed
-
- Rombaux P, Potier H, Markessis E, Duprez T, Hummel T. Olfactory bulb volume and depth of olfactory sulcus in patients with idiopathic olfactory loss. Eur Arch Otorhinolaryngol. 2010;267:1551–1556. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
