

Clinical, socioeconomic, and behavioural factors at age 50 years and risk of cardiometabolic multimorbidity and mortality: A cohort study
- PMID: 29782486
- PMCID: PMC5962054
- DOI: 10.1371/journal.pmed.1002571
Clinical, socioeconomic, and behavioural factors at age 50 years and risk of cardiometabolic multimorbidity and mortality: A cohort study
Abstract
Background: Multimorbidity is increasingly common and is associated with adverse health outcomes, highlighting the need to broaden the single-disease framework that dominates medical research. We examined the role of midlife clinical characteristics, socioeconomic position, and behavioural factors in the development of cardiometabolic multimorbidity (at least 2 of diabetes, coronary heart disease, and stroke), along with how these factors modify risk of mortality.
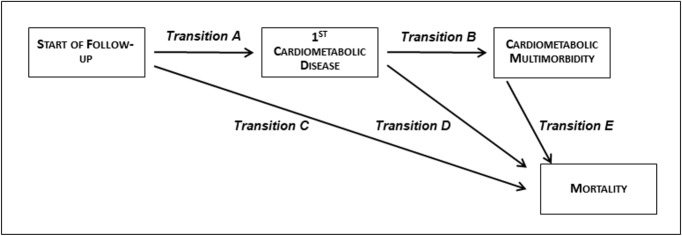
Methods and findings: Data on 8,270 men and women were drawn from the Whitehall II cohort study, with mean follow-up of 23.7 years (1985 to 2017). Three sets of risk factors were assessed at age 50 years, each on a 5-point scale: clinical profile (hypertension, hypercholesterolemia, overweight/obesity, family history of cardiometabolic disease), occupational position, and behavioural factors (smoking, alcohol consumption, diet, physical activity). The outcomes examined were cardiometabolic disease (diabetes, coronary heart disease, stroke), cardiometabolic multimorbidity, and mortality. We used multi-state models to examine the role of risk factors in 5 components of the cardiometabolic disease trajectory: from healthy state to first cardiometabolic disease, from first cardiometabolic disease to cardiometabolic multimorbidity, from healthy state to death, from first cardiometabolic disease to death, and from cardiometabolic multimorbidity to death. A total of 2,501 participants developed 1 of the 3 cardiometabolic diseases, 511 developed cardiometabolic multimorbidity, and 1,406 died. When behavioural and clinical risk factors were considered individually, only smoking was associated with all five transitions. In a model containing all 3 risk factor scales, midlife clinical profile was the strongest predictor of first cardiometabolic disease (hazard ratio for the least versus most favourable profile: 3.74; 95% CI: 3.14-4.45) among disease-free participants. Among participants with 1 cardiometabolic disease, adverse midlife socioeconomic (1.54; 95% CI: 1.10-2.15) and behavioural factors (2.00; 95% CI: 1.40-2.85), but not clinical characteristics, were associated with progression to cardiometabolic multimorbidity. Only midlife behavioural factors predicted mortality among participants with cardiometabolic disease (2.12; 95% CI: 1.41-3.18) or cardiometabolic multimorbidity (3.47; 95% CI: 1.81-6.66). A limitation is that the study was not large enough to estimate transitions between each disease and subsequent outcomes and between all possible pairs of diseases.
Conclusions: The importance of specific midlife factors in disease progression, from disease-free state to single disease, multimorbidity, and death, varies depending on the disease stage. While clinical risk factors at age 50 determine the risk of incident cardiometabolic disease in a disease-free population, midlife socioeconomic and behavioural factors are stronger predictors of progression to multimorbidity and mortality in people with cardiometabolic disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Bayliss EA, Edwards AE, Steiner JF, Main DS. Processes of care desired by elderly patients with multimorbidities. Fam Pract. 2008;25(4):287–93. doi: 10.1093/fampra/cmn040 - DOI - PMC - PubMed
-
- Agborsangaya CB, Lau D, Lahtinen M, Cooke T, Johnson JA. Multimorbidity prevalence and patterns across socioeconomic determinants: a cross-sectional survey. BMC Public Health. 2012;12:201 doi: 10.1186/1471-2458-12-201 - DOI - PMC - PubMed
-
- McLean G, Gunn J, Wyke S, Guthrie B, Watt GC, Blane DN, et al. The influence of socioeconomic deprivation on multimorbidity at different ages: a cross-sectional study. Br J Gen Pract. 2014;64(624):e440–7. doi: 10.3399/bjgp14X680545 - DOI - PMC - PubMed
-
- Emerging Risk Factors Collaboration, Di Angelantonio E, Kaptoge S, Wormser D, Willeit P, Butterworth AS, et al. Association of cardiometabolic multimorbidity with mortality. JAMA. 2015;314(1):52–60. doi: 10.1001/jama.2015.7008 - DOI - PMC - PubMed
-
- Weiss CO, Boyd CM, Yu Q, Wolff JL, Leff B. Patterns of prevalent major chronic disease among older adults in the United States. JAMA. 2007;298(10):1160–2. doi: 10.1001/jama.298.10.1160-b - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
