

Prolonged and large outbreak of invasive group A Streptococcus disease within a nursing home: repeated intrafacility transmission of a single strain
- PMID: 29783026
- PMCID: PMC6500455
- DOI: 10.1016/j.cmi.2018.04.034
Prolonged and large outbreak of invasive group A Streptococcus disease within a nursing home: repeated intrafacility transmission of a single strain
Abstract
Objectives: Multiple invasive group A Streptococcus (GAS) infections were reported to public health by a skilled nursing facility (facility A) in Illinois between May 2014 and August 2016. Cases continued despite interventions including antibiotic prophylaxis for all residents and staff. Two other geographically close facilities reported contemporaneous outbreaks of GAS. We investigated potential reasons for ongoing transmission.
Methods: We obtained epidemiologic data from chart review of cases and review of facility and public health records from previous investigations into the outbreak. Infection control practices at facility A were observed and evaluated. Whole genome sequencing followed by phylogenetic analysis was performed on available isolates from the three facilities.
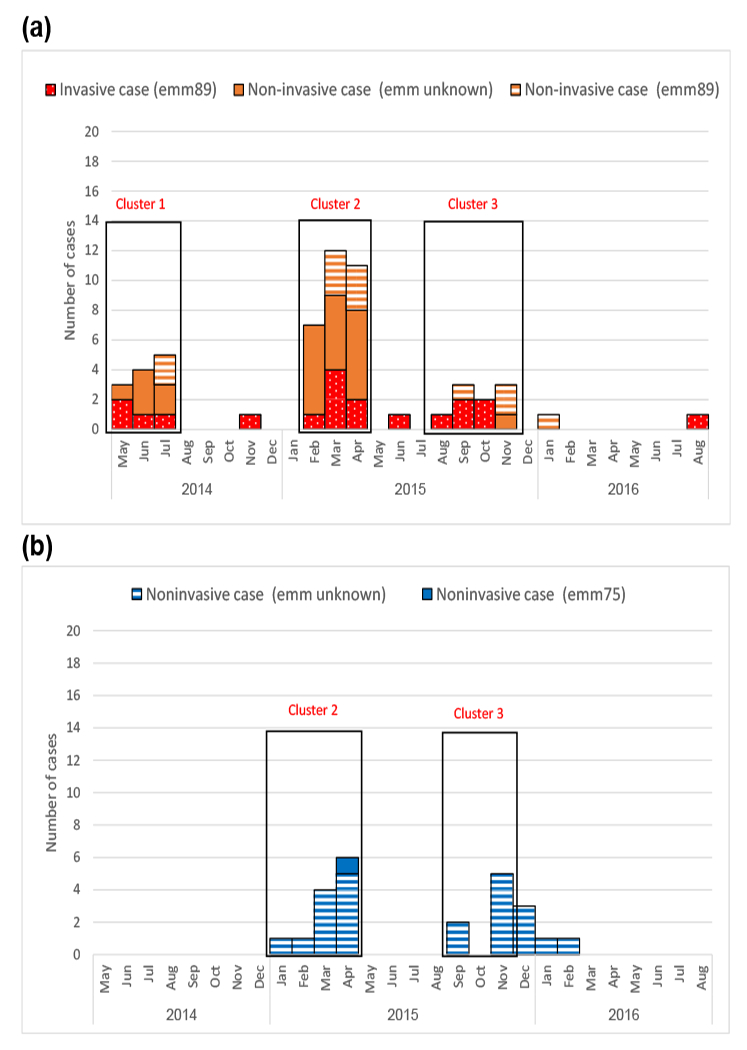
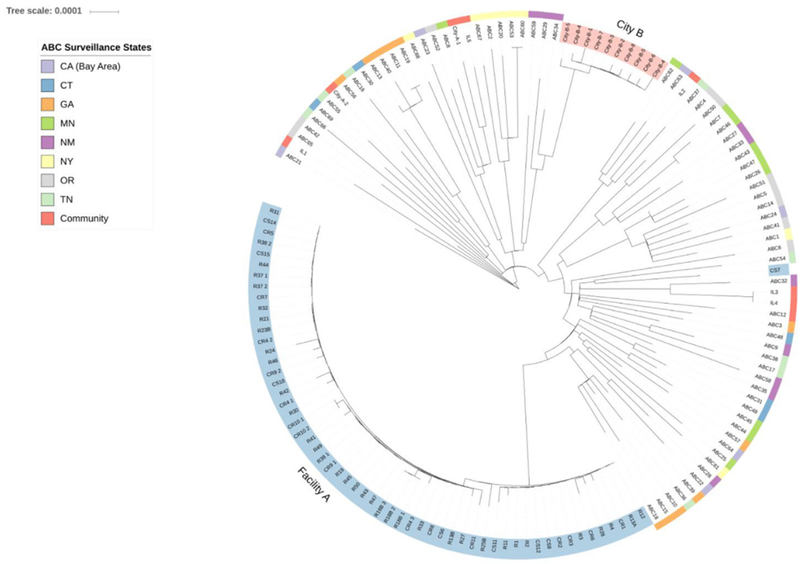
Results: From 2014 to 2016, 19 invasive and 60 noninvasive GAS infections were identified at facility A occurring in three clusters. Infection control evaluations during clusters 2 and 3 identified hand hygiene compliance rates of 14% to 25%, appropriate personal protective equipment use in only 33% of observed instances, and deficient wound-care practices. GAS isolates from residents and staff of all three facilities were subtype emm89.0; on phylogenetic analysis, facility A isolates were monophyletic and distinct.
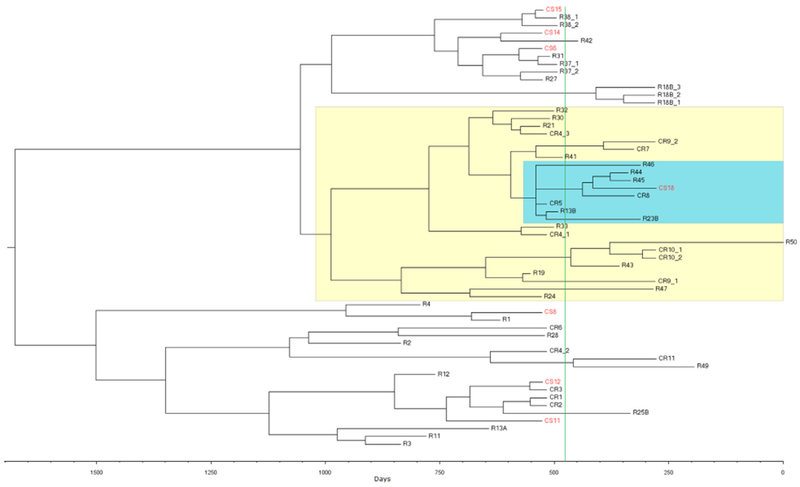
Conclusions: Inadequate infection control and improper wound-care practices likely led to this 28-month-long outbreak of severe infections in a skilled nursing facility. Whole genome sequencing and phylogenetic analysis suggested that intrafacility transmission of a single highly transmissible GAS strain was responsible for the outbreak in facility A. Integration of genomic epidemiology tools with traditional epidemiology and infection control assessments was helpful in investigation of a facility-wide outbreak.
Keywords: Group A; Intrafacility transmission; Invasive; Outbreak; Single strain; Streptococcal disease.
Published by Elsevier Ltd.
Figures
Comment in
-
Critical Infection Control Adaptations to Survive COVID-19 in Retirement Communities.J Gerontol Nurs. 2020 Jun 1;46(6):3-5. doi: 10.3928/00989134-20200511-03. J Gerontol Nurs. 2020. PMID: 32453432 No abstract available.
References
-
- Centers for Disease Control and Prevention. Active bacterial core surveillance (ABCs), Emerging Infections Program Network, group A Streptococcus surveillance report—2014. Available at: http://www.cdc.gov/abcs/reports-findings/survreports/gas14.pdf.
-
- Ht Jordan, Richards CL Jr Burton DC, Thigpen MC Van Beneden CA. Group A streptococcal disease in long-term care facilities: descriptive epidemiology and potential control measures. Clin Infect Dis 2007;45:742–52. - PubMed
-
- Spellerberg B, Brandt C. Laboratory diagnosis of Streptococcus pyogenes (group A streptococci) In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes: basic biology to clinical manifestations. Oklahoma City, OK: University of Oklahoma Health Sciences Center; 2016. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
