

A meta-analysis of the effect of a dexamethasone intravitreal implant versus intravitreal anti-vascular endothelial growth factor treatment for diabetic macular edema
- PMID: 29784048
- PMCID: PMC5963018
- DOI: 10.1186/s12886-018-0779-1
A meta-analysis of the effect of a dexamethasone intravitreal implant versus intravitreal anti-vascular endothelial growth factor treatment for diabetic macular edema
Abstract
Background: This meta-analysis evaluated the effectiveness and safety of dexamethasone (DEX) implant and intravitreal anti-vascular endothelial growth factor (VEGF) treatment for diabetic macular edema (DME).
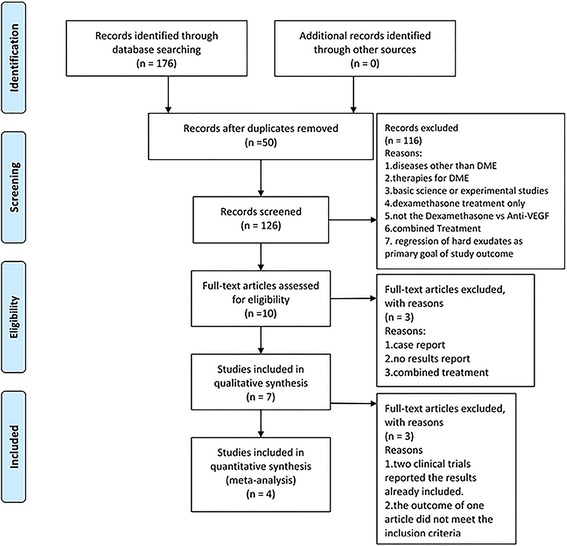
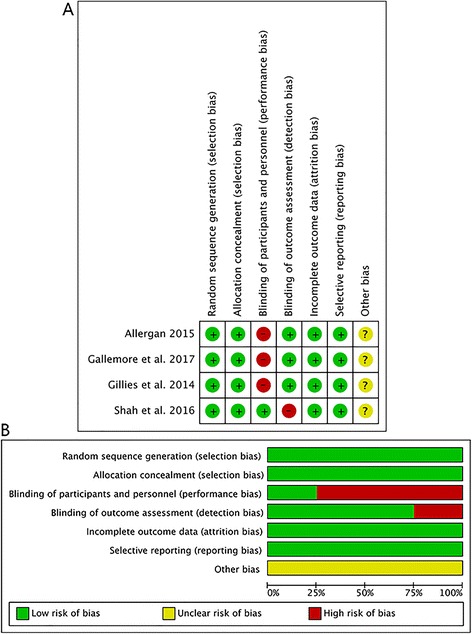
Methods: The PubMed, Embase, clinicaltrials.gov website and Cochrane Library databases were comprehensively searched for studies comparing DEX implant with anti-VEGF in patients with DME. Best-corrected visual acuity (BCVA), central subfield thickness (CST) and adverse events were extracted from the final eligible studies. Review Manager (RevMan) 5.3 for Mac was used to analyze the data and GRADE profiler were used to access the quality of outcomes.
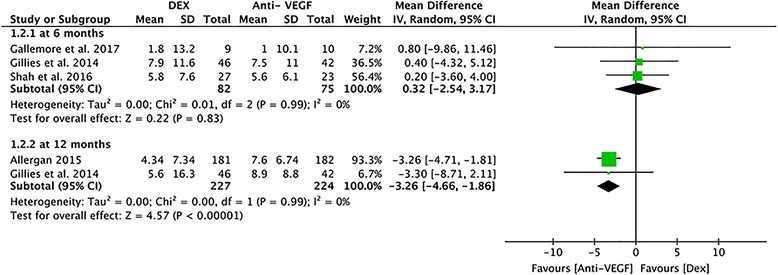
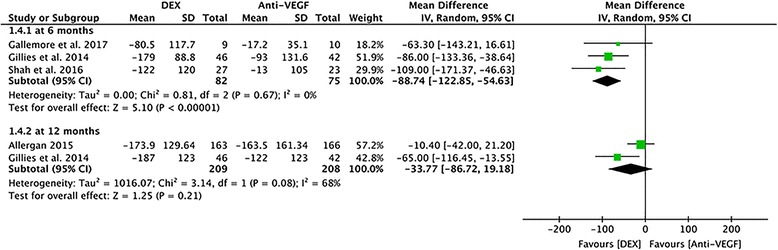
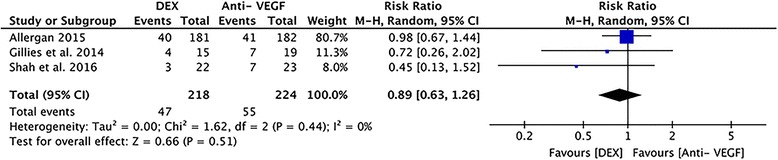
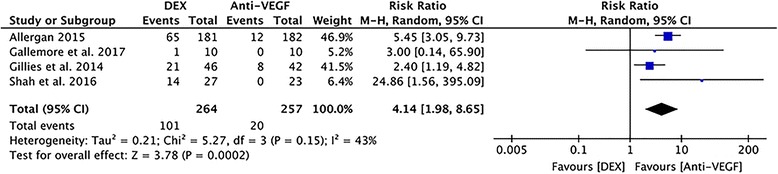
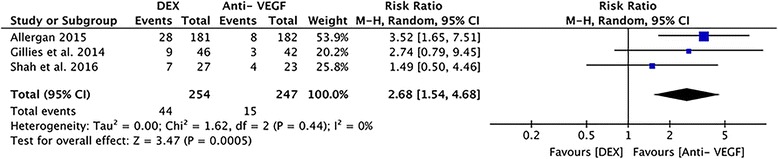
Results: Based on four randomized clinical trials assessing a total of 521 eyes, the DEX implant can achieve visual acuity improvement for DME at rates similar to those achieved via anti-VEGF treatment (mean difference [MD] = - 0.43, P = 0.35), with superior anatomic outcomes at 6 months (MD = - 86.71 μm, P = 0.02), while requiring fewer injections, in comparison to anti-VEGF treatment. Although the mean reduction in CST did not showed significant difference at 12 months (MD = - 33.77 μm, P = 0.21), the significant in BCVA from baseline to 12 months supported the anti-VEGF treatment (MD = - 3.26, P < 0.00001). No statistically significant differences in terms of the serious adverse events. However, use of the DEX implant has higher risk of intraocular pressure elevation and cataract than anti-VEGF treatment.
Conclusions: Compared with anti-VEGF, DEX implant improved anatomical outcomes significantly. However, this did not translate to improved visual acuity, which may be due to the progression of cataract. Therefore, the DEX implant may be recommended as a first chioce for select cases, such as for pseudophakic eyes, anti-VEGF-resistant eyes, or patients reluctant to receive intravitreal injections frequently.
Keywords: Anti-VEGF; Dexamethasone implant; Diabetic macular edema; Meta-analysis; Ozurdex.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Patz A, Schatz H, Berkow JW, Gittelsohn AM, Ticho U. Macular edema--an overlooked complication of diabetic retinopathy. Trans Am Acad Ophthalmol Otolaryngol. 1973;77:Op34–Op42. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
