

Randomized Trial Comparing Open Radical Cystectomy and Robot-assisted Laparoscopic Radical Cystectomy: Oncologic Outcomes
- PMID: 29784190
- PMCID: PMC6697266
- DOI: 10.1016/j.eururo.2018.04.030
Randomized Trial Comparing Open Radical Cystectomy and Robot-assisted Laparoscopic Radical Cystectomy: Oncologic Outcomes
Abstract
Background: Open radical cystectomy (ORC) has proven to be an important component in the treatment of high-risk bladder cancer (BCa). ORC surgical morbidity remains high; therefore, minimally invasive surgical techniques have been introduced in an attempt to improve patient outcomes.
Objective: To compare cancer outcomes in BCa patients managed with ORC or robotic-assisted radical cystectomy (RARC).
Design, setting, and participants: A prospective, randomized trial was completed between 2010 and 2013. Patients were randomized to ORC/pelvic lymphadenectomy (PLND) or RARC/PLND, with all undergoing open/extracorporeal urinary diversion. Median follow-up was 4.9 (IQR: 3.9-5.9) yr after surgery among surviving patients.
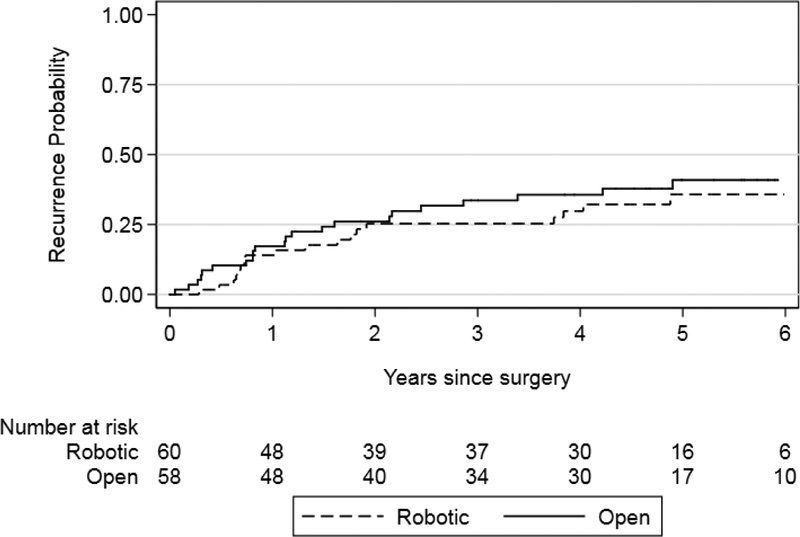
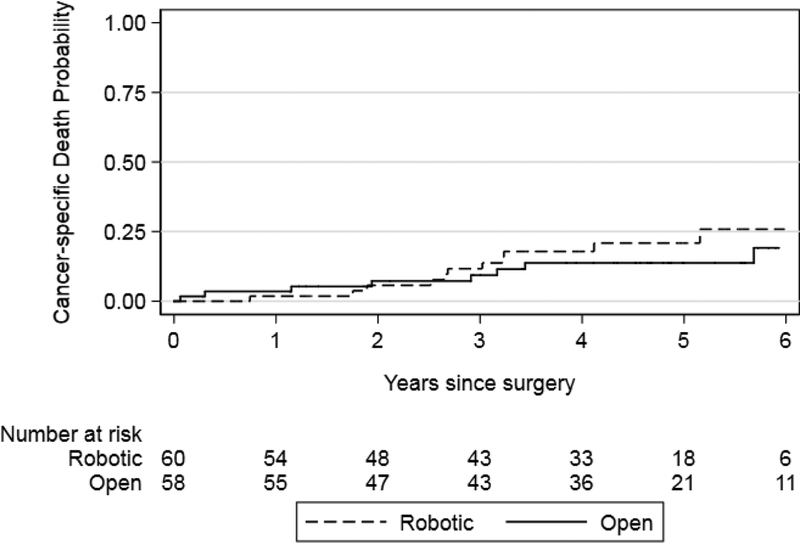
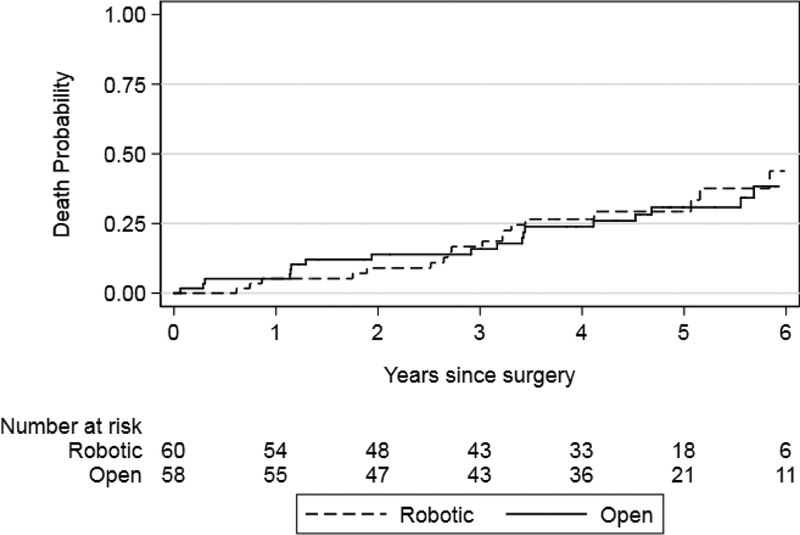
Outcome measurements and statistical analysis: Secondary outcomes to the trial included recurrence-free, cancer-specific, and overall survival.
Results and limitations: The trial randomized 118 patients who underwent RC/PLND and urinary diversion. Sixty were randomized to RARC and 58 to ORC. Four RARC-assigned patients refused randomization and received ORC; however, an intention to treat analysis was performed. No differences were observed in recurrence (hazard ratio [HR]: 1.27; 95% confidence interval [CI]: 0.69-2.36; p=0.4) or cancer-specific survival (p=0.4). No difference in overall survival was observed (p=0.8). However, the pattern of first recurrence demonstrated a nonstatistically significant increase in metastatic sites for those undergoing ORC (sub-HR [sHR]: 2.21; 95% CI: 0.96-5.12; p=0.064) and a greater number of local/abdominal sites in the RARC-treated patients (sHR: 0.34; 95% CI: 0.12-0.93; p=0.035). The major limitation to this study is that the trial was not powered to determine differences in cancer recurrences, survival outcomes, or patterns of recurrence.
Conclusions: The secondary outcomes from our randomized trial did not definitively demonstrate differences in cancer outcomes in patients treated with ORC or RARC. However, differences in observed patterns of first recurrence highlight the need for future studies.
Patient summary: Of 118 patients randomly assigned to undergo radical cystectomy/pelvic lymphadenectomy and urinary diversion, half were assigned to open surgery and half to robot-assisted techniques. We found no difference in risk of recurring or dying of bladder cancer between the two groups.
Keywords: Bladder cancer; Radical cystectomy; Robotics.
Copyright © 2018 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Robotic Cystectomy-Moving from Innovation to Measurable Impact.Eur Urol. 2018 Oct;74(4):472-473. doi: 10.1016/j.eururo.2018.05.028. Epub 2018 Jun 10. Eur Urol. 2018. PMID: 29898834
-
Will long term oncologic follow-up make the case for robotic assisted radical cystectomy?Transl Androl Urol. 2018 Dec;7(Suppl 6):S696-S698. doi: 10.21037/tau.2018.11.01. Transl Androl Urol. 2018. PMID: 30687598 Free PMC article. No abstract available.
-
Does robotic radical cystectomy impede oncological outcome in bladder cancer patients?Transl Androl Urol. 2018 Dec;7(Suppl 6):S744-S746. doi: 10.21037/tau.2018.08.16. Transl Androl Urol. 2018. PMID: 30687614 Free PMC article. No abstract available.
-
Reply to Siebren Dijkstra and Carl J. Wijburg's Letter to the Editor re: Bernard H. Bochner, Guido Dalbagni, Karim H. Marzouk, et al. Randomized Trial Comparing Open Radical Cystectomy and Robot-assisted Laparoscopic Radical Cystectomy: Oncologic Outcomes. Eur Urol 2018;74:465-71. Can the Pattern of Cancer Recurrence Truly be Assigned to the Surgical Modality?Eur Urol. 2019 May;75(5):e138-e139. doi: 10.1016/j.eururo.2019.01.037. Epub 2019 Feb 1. Eur Urol. 2019. PMID: 30712972 No abstract available.
-
Re: Bernard H. Bochner, Guido Dalbagni, Karim H. Marzouk, et al. Randomized Trial Comparing Open Radical Cystectomy and Robot-assisted Laparoscopic Radical Cystectomy: Oncologic Outcomes. Eur Urol 2018;74:465-71: Can the Pattern of Cancer Recurrence Truly be Assigned to the Surgical Modality?Eur Urol. 2019 May;75(5):e137. doi: 10.1016/j.eururo.2019.01.036. Epub 2019 Feb 2. Eur Urol. 2019. PMID: 30723049 No abstract available.
References
-
- Bochner BH, Kattan MW, Vora KC. Postoperative nomogram predicting risk of recurrence after radical cystectomy for bladder cancer. J Clin Oncol 2006;24:3967–72. - PubMed
-
- Stein JP, Lieskovsky G, Cote R, et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol 2001;19:666–75. - PubMed
-
- Johar RS, Hayn MH, Stegemann AP, et al. Complications after robot-assisted radical cystectomy: results from the International Robotic Cystectomy Consortium. Eur Urol 2013;64:52–7. - PubMed
-
- Nazmy M, Yuh B, Kawachi M, et al. Early and late complications of robot-assisted radical cystectomy: a standardized analysis by urinary diversion type. J Urol 2014;191:681–7. - PubMed
-
- Wechter ME, Mohd J, Magrina JF, et al. Complications in robotic-assisted gynecologic surgery according to case type: a 6-year retrospective cohort study using Clavien-Dindo classification. J Minim Invasive Gynecol 2014;21:844–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
