

Incidences of Pseudomonas aeruginosa-Associated Ventilator-Associated Pneumonia within Studies of Respiratory Tract Applications of Polymyxin: Testing the Stoutenbeek Concurrency Postulates
- PMID: 29784844
- PMCID: PMC6105782
- DOI: 10.1128/AAC.00291-18
Incidences of Pseudomonas aeruginosa-Associated Ventilator-Associated Pneumonia within Studies of Respiratory Tract Applications of Polymyxin: Testing the Stoutenbeek Concurrency Postulates
Abstract
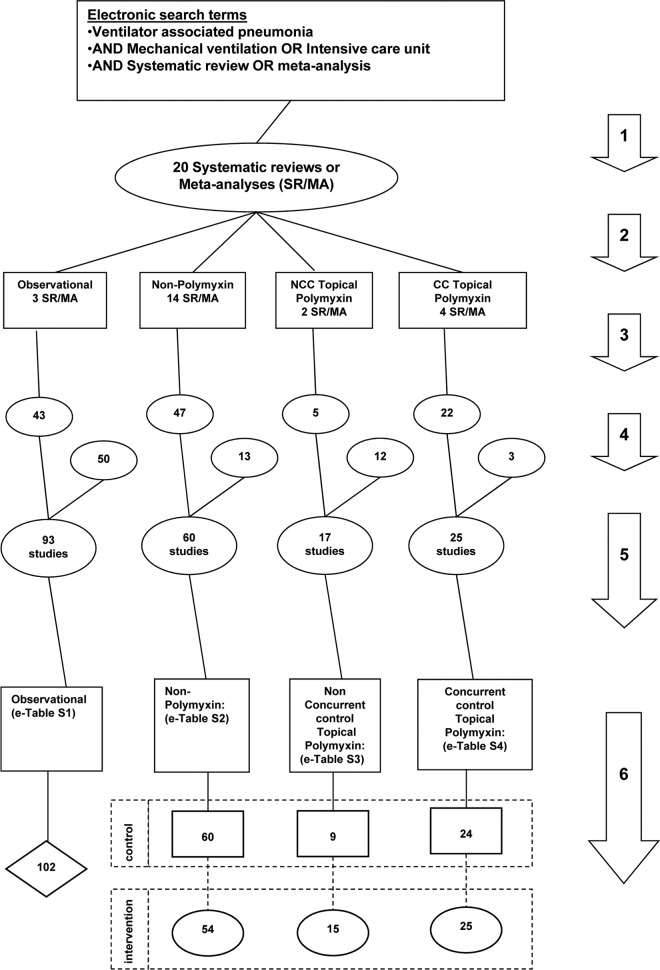
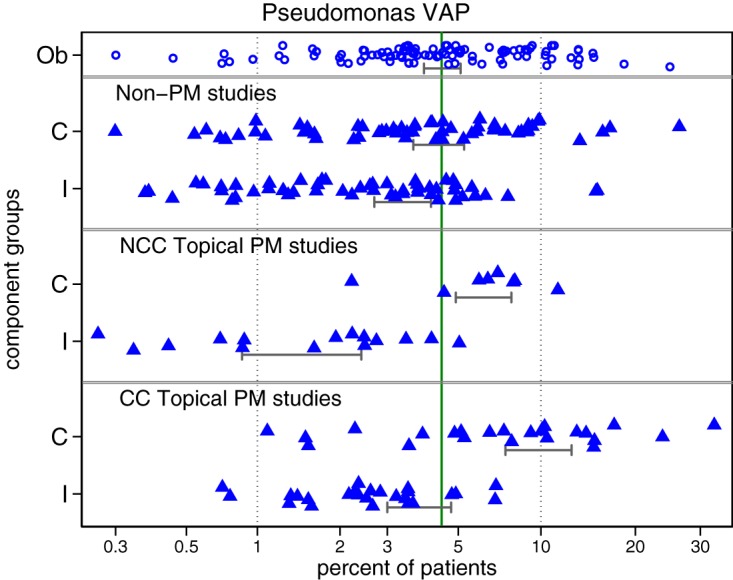
Regimens containing topical polymyxin appear highly effective at preventing ventilator-associated pneumonia (VAP) overall and, more so, VAP caused by Gram-negative bacteria. However, Stoutenbeek's postulates that VAP incidences within studies of topical antibiotics depend on the context of whether the component (control and intervention) groups of each study were concurrent versus nonconcurrent remain untested. The literature was searched for concurrent control (CC) versus nonconcurrent control (NCC) designed studies of respiratory tract applications of topical polymyxin to mechanically ventilated (MV) patients that reported incidences of Pseudomonas-associated ventilator-associated pneumonia (PsVAP). Studies of various interventions other than topical polymyxin (nonpolymyxin studies) served to provide additional points of reference. The PsVAP incidences within the component groups of all studies were benchmarked against groups from observational studies. This was undertaken by meta-regression using generalized estimating equation methods. Dot plots, caterpillar plots, and funnel plots enable visual benchmarking. The PsVAP benchmark (and 95% confidence interval [CI]) derived from 102 observational groups is 4.6% (4.0 to 5.3%). In contrast, the mean PsVAP within NCC polymyxin intervention groups (1.6%; CI, 1.0 to 4.5%) is lower than that of all other component group categories. The mean PsVAP within CC polymyxin control groups (9.9%; CI, 7.6 to 12.8%) is higher than that of all other component group categories. The PsVAP incidences of control and intervention groups of studies of respiratory tract applications of polymyxin are dependent on whether the groups were within a concurrent versus nonconcurrent study. Stoutenbeek's concurrency postulates are validated.
Keywords: Pseudomonas; antibiotic prophylaxis; intensive care; mechanical ventilation; polymyxin; selective digestive decontamination; study design; ventilator-associated pneumonia.
Copyright © 2018 American Society for Microbiology.
Figures
References
-
- de Smet AMGA, Kluytmans JAJW, Cooper BS, Mascini EM, Benus RFJ, van der Werf TS, van der Hoeven JG, Pickkers P, Bogaers-Hofman D, van der Meer NJ, Bernards AT, Kuijper EJ, Joore JC, Leverstein-van Hall MA, Bindels AJ, Jansz AR, Wesselink RM, de Jongh BM, Dennesen PJ, van Asselt GJ, te Velde LF, Frenay IH, Kaasjager K, Bosch FH, van Iterson M, Thijsen SF, Kluge GH, Pauw W, de Vries JW, Kaan JA, Arends JP, Aarts LP, Sturm PD, Harinck HI, Voss A, Uijtendaal EV, Blok HE, Thieme Groen ES, Pouw ME, Kalkman CJ, Bonten MJ. 2009. Decontamination of the digestive tract and oropharynx in ICU patients. N Engl J Med 360:20–31. doi: 10.1056/NEJMoa0800394. - DOI - PubMed
-
- Pileggi C, Bianco A, Flotta D, Nobile CG, Pavia M. 2011. Prevention of ventilator-associated pneumonia, mortality and all intensive care unit acquired infections by topically applied antimicrobial or antiseptic agents: a meta-analysis of randomized controlled trials in intensive care units. Crit Care 15:R155. doi: 10.1186/cc10285. - DOI - PMC - PubMed
-
- Silvestri L, Van Saene HK, Casarin A, Berlot G, Gullo A. 2008. Impact of selective decontamination of the digestive tract on carriage and infection due to Gram-negative and Gram-positive bacteria: a systematic review of randomised controlled trials. Anaesth Intensive Care 36:324–338. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
