

A retrospective histological comparison of EUS-guided fine-needle biopsy using a novel franseen needle and a conventional end-cut type needle
- PMID: 29786033
- PMCID: PMC6400082
- DOI: 10.4103/eus.eus_11_18
A retrospective histological comparison of EUS-guided fine-needle biopsy using a novel franseen needle and a conventional end-cut type needle
Abstract
Background and objectives: Recently, a 22G Franseen needle for EUS-guided fine-needle biopsy (EUS-FNB) with three novel symmetric heels has been developed to adequately obtain a core tissue.
Methods: All 38 consecutive patients with pancreatic masses who underwent EUS-FNB using a Franseen needle were investigated retrospectively to assess the efficacy and safety of EUS-FNB using the Franseen needle. Then, the EUS-FNB outcomes and histological assessments of the tissue obtained by EUS-FNB using the Franseen needle and EUS-FNA using the conventional end-cut type needle for each of the 30 pancreatic ductal adenocarcinoma cases were compared.
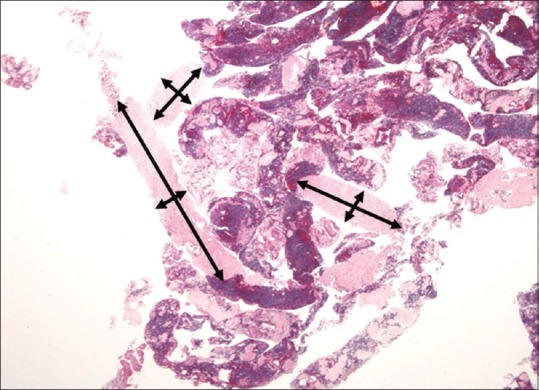
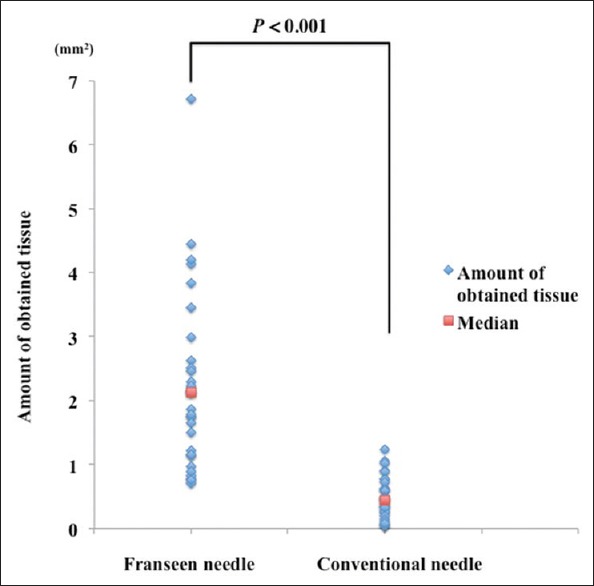
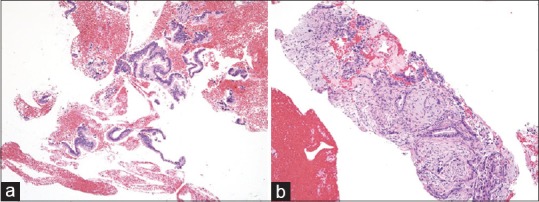
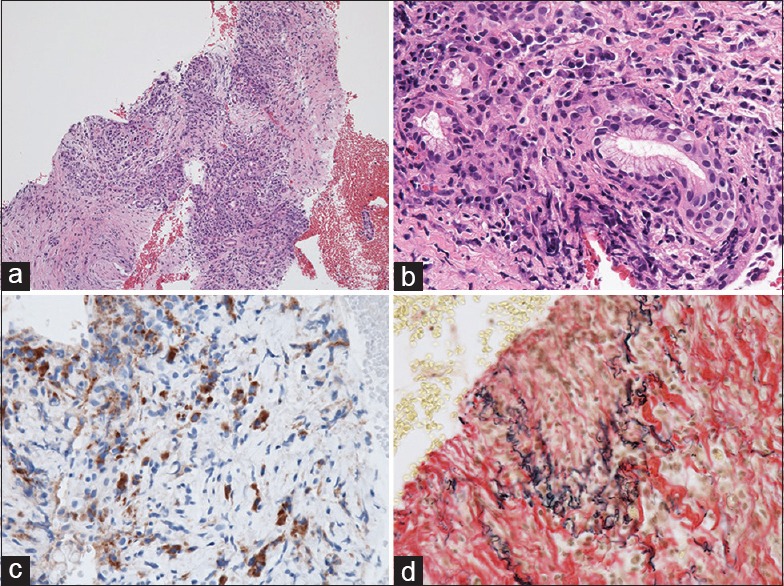
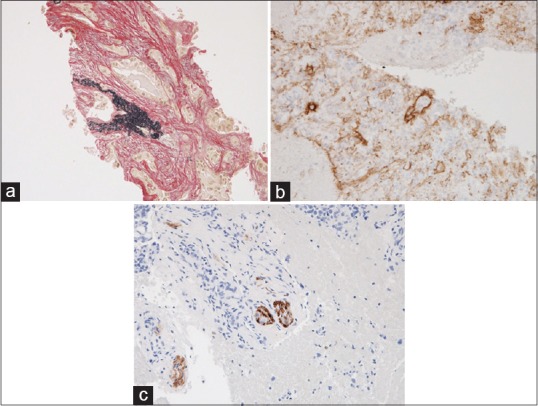
Results: An accurate histological diagnosis of the Franseen needle was achieved with a mean of 2 passes in 97.4% of patients. Although the accurate histological diagnosis rate of pancreatic ductal adenocarcinoma was not significantly different (96.7% vs. 93.3%, P = 0.55), the mean number of passes in the Franseen needle was significantly less than that in the conventional needle (2.1 ± 0.4 vs. 3.2 ± 0.8, P < 0.001). The presence of desmoplastic fibrosis with neoplastic cellular elements and venous invasion were significantly higher (96.7% vs. 40.0%, P < 0.001 and 23.3% vs. 0%, P < 0.01, respectively) and the amount of obtained tissue was significantly larger with the Franseen needle (2.13 mm2 vs. 0.45 mm2, P < 0.001).
Conclusions: EUS-FNB using the Franseen needle enables the acquisition of a larger amount of tissue sample and achieves an accurate histological diagnosis with a smaller number of passes than the conventional end-cut type needle.
Keywords: Endoscopic ultrasound; fine needle biopsy; histology; pancreatic cancer.
Conflict of interest statement
None
Figures

References
-
- Binmoeller KF, Thul R, Rathod V, et al. Endoscopic ultrasound-guided, 18-gauge, fine needle aspiration biopsy of the pancreas using a 2.8 mm channel convex array echoendoscope. Gastrointest Endosc. 1998;47:121–7. - PubMed
-
- Itoi T, Tsuchiya T, Itokawa F, et al. Histological diagnosis by EUS-guided fine-needle aspiration biopsy in pancreatic solid masses without on-site cytopathologist: A single-center experience. Dig Endosc. 2011;23(Suppl 1):34–8. - PubMed
-
- Wani S, Muthusamy VR, Komanduri S. EUS-guided tissue acquisition: An evidence-based approach (with videos) Gastrointest Endosc. 2014;80:939–59. e7. - PubMed
-
- Bang JY, Hawes R, Varadarajulu S. A meta-analysis comparing proCore and standard fine-needle aspiration needles for endoscopic ultrasound-guided tissue acquisition. Endoscopy. 2016;48:339–49. - PubMed
-
- Huang JY, Chang KJ. Improvements and innovations in endoscopic ultrasound guided fine needle aspiration. J Hepatobiliary Pancreat Sci. 2015;22:E37–46. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
