

Mycoplasma pneumoniae Among Children Hospitalized With Community-acquired Pneumonia
- PMID: 29788037
- PMCID: PMC6552676
- DOI: 10.1093/cid/ciy419
Mycoplasma pneumoniae Among Children Hospitalized With Community-acquired Pneumonia
Abstract
Background: The epidemiology of Mycoplasma pneumoniae (Mp) among US children (<18 years) hospitalized with community-acquired pneumonia (CAP) is poorly understood.
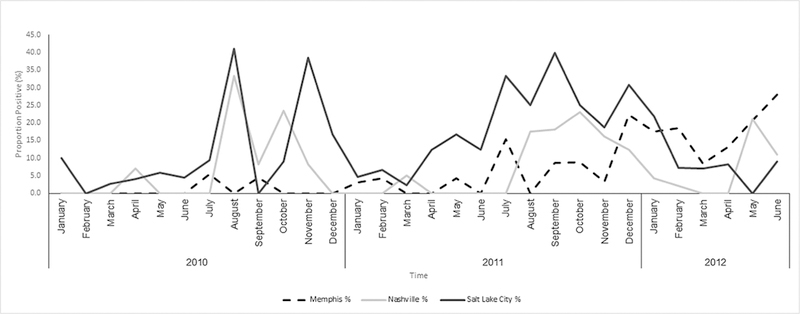
Methods: In the Etiology of Pneumonia in the Community study, we prospectively enrolled 2254 children hospitalized with radiographically confirmed pneumonia from January 2010-June 2012 and tested nasopharyngeal/oropharyngeal swabs for Mp using real-time polymerase chain reaction (PCR). Clinical and epidemiological features of Mp PCR-positive and -negative children were compared using logistic regression. Macrolide susceptibility was assessed by genotyping isolates.
Results: One hundred and eighty two (8%) children were Mp PCR-positive (median age, 7 years); 12% required intensive care and 26% had pleural effusion. No in-hospital deaths occurred. Macrolide resistance was found in 4% (6/169) isolates. Of 178 (98%) Mp PCR-positive children tested for copathogens, 50 (28%) had ≥1 copathogen detected. Variables significantly associated with higher odds of Mp detection included age (10-17 years: adjusted odds ratio [aOR], 10.7 [95% confidence interval {CI}, 5.4-21.1] and 5-9 years: aOR, 6.4 [95% CI, 3.4-12.1] vs 2-4 years), outpatient antibiotics ≤5 days preadmission (aOR, 2.3 [95% CI, 1.5-3.5]), and copathogen detection (aOR, 2.1 [95% CI, 1.3-3.3]). Clinical characteristics were non-specific.
Conclusions: Usually considered as a mild respiratory infection, Mp was the most commonly detected bacteria among children aged ≥5 years hospitalized with CAP, one-quarter of whom had codetections. Although associated with clinically nonspecific symptoms, there was a need for intensive care in some cases. Mycoplasma pneumoniae should be included in the differential diagnosis for school-aged children hospitalized with CAP.
Figures
Comment in
-
Mycoplasma pneumoniae as a Cause of Community-Acquired Pneumonia in Children.Clin Infect Dis. 2019 Jan 1;68(1):13-14. doi: 10.1093/cid/ciy421. Clin Infect Dis. 2019. PMID: 29788200 No abstract available.
References
-
- Bitnun A, Ford-Jones EL, Petric M, et al. Acute childhood encephalitis and Mycoplasma pneumoniae. Clin Infect Dis 2001; 32:1674–84. - PubMed
-
- Daxboeck F, Blacky A, Seidl R, Krause R, Assadian O. Diagnosis, treatment, and prognosis of Mycoplasma pneumoniae childhood encephalitis: systematic review of 58 cases. J Child Neurol 2004; 19:865–71. - PubMed
-
- Meyer Sauteur PM, Streuli JC, Iff T, Goetschel P. Mycoplasma pneumoniae-associated encephalitis in childhood-nervous system disorder during or after a respiratory tract infection. Klin Padiatr 2011; 223:209–13. - PubMed
-
- Meyer Sauteur PM, Goetschel P, Lautenschlager S. Mycoplasma pneumoniae and mucositis—part of the Stevens-Johnson syndrome spectrum. J Dtsch Dermatol Ges 2012; 10:740–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
