

Haemodynamics, dyspnoea, and pulmonary reserve in heart failure with preserved ejection fraction
- PMID: 29788047
- PMCID: PMC6658816
- DOI: 10.1093/eurheartj/ehy268
Haemodynamics, dyspnoea, and pulmonary reserve in heart failure with preserved ejection fraction
Abstract
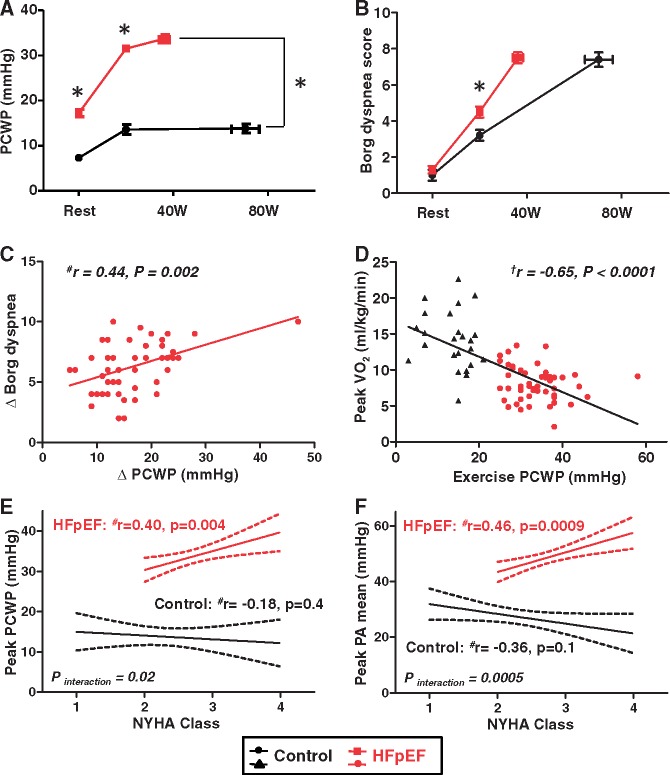
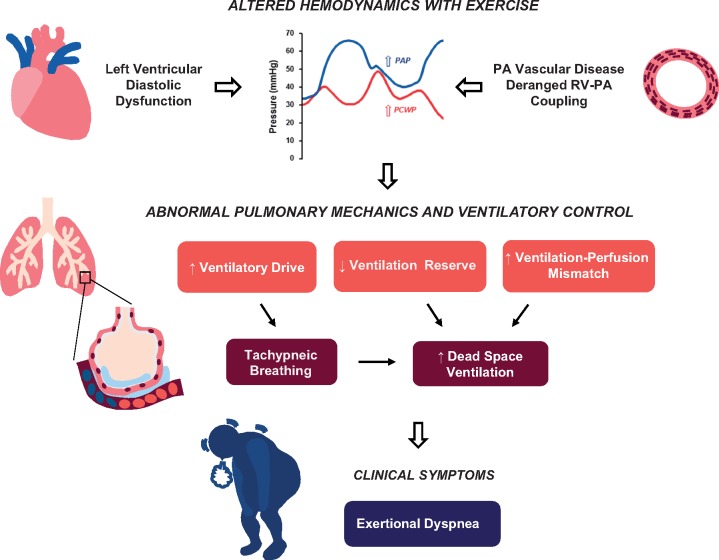
Aims: Increases in left ventricular filling pressure are a fundamental haemodynamic abnormality in heart failure with preserved ejection fraction (HFpEF). However, very little is known regarding how elevated filling pressures cause pulmonary abnormalities or symptoms of dyspnoea. We sought to determine the relationships between simultaneously measured central haemodynamics, symptoms, and lung ventilatory and gas exchange abnormalities during exercise in HFpEF.
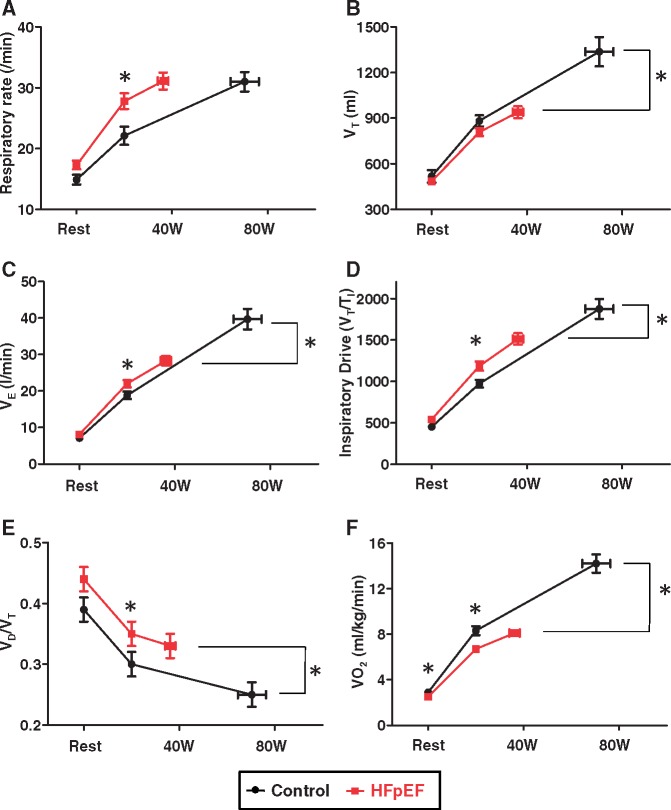
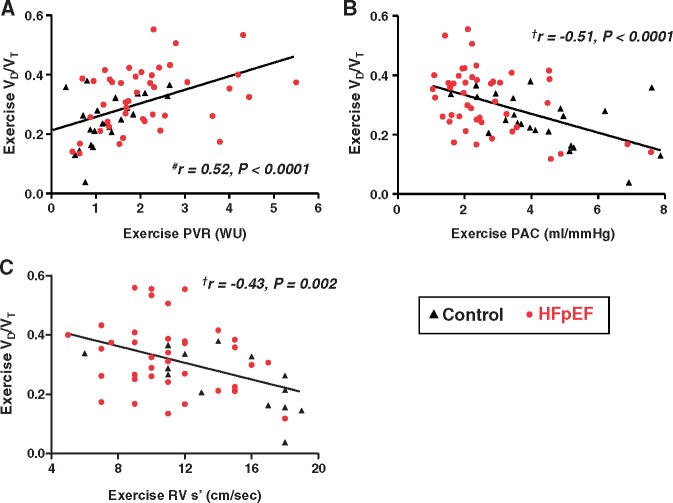
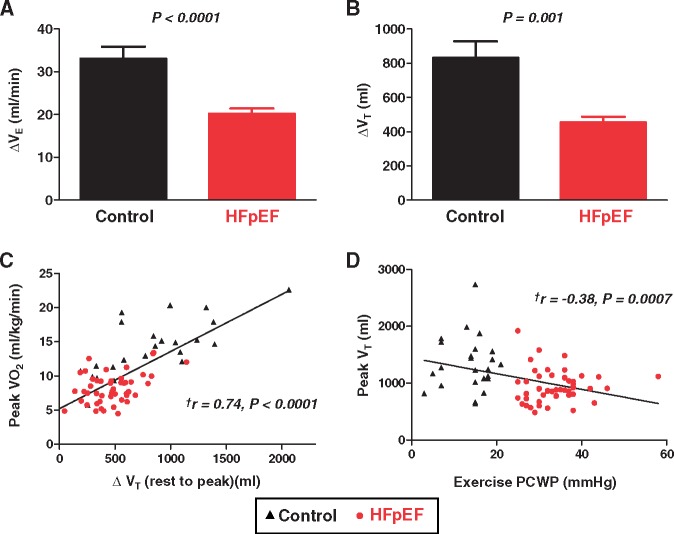
Methods and results: Subjects with invasively-proven HFpEF (n = 50) and non-cardiac causes of dyspnoea (controls, n = 24) underwent cardiac catheterization at rest and during exercise with simultaneous expired gas analysis. During submaximal (20 W) exercise, subjects with HFpEF displayed higher pulmonary capillary wedge pressures (PCWP) and pulmonary artery pressures, higher Borg perceived dyspnoea scores, and increased ventilatory drive and respiratory rate. At peak exercise, ventilation reserve was reduced in HFpEF compared with controls, with greater dead space ventilation (higher VD/VT). Increasing exercise PCWP was directly correlated with higher perceived dyspnoea scores, lower peak exercise capacity, greater ventilatory drive, worse New York Heart Association (NYHA) functional class, and impaired pulmonary ventilation reserve.
Conclusion: This study provides the first evidence linking altered exercise haemodynamics to pulmonary abnormalities and symptoms of dyspnoea in patients with HFpEF. Further study is required to identify the mechanisms by which haemodynamic derangements affect lung function and symptoms and to test novel therapies targeting exercise haemodynamics in HFpEF.
Figures
Comment in
-
Questioning the obvious: does dyspnoea really matter in heart failure?Eur Heart J. 2018 Aug 7;39(30):2822-2824. doi: 10.1093/eurheartj/ehy354. Eur Heart J. 2018. PMID: 29939237 No abstract available.
References
-
- Reddy YN, Borlaug BA.. Heart failure with preserved ejection fraction. Curr Probl Cardiol 2016;41:145–188. - PubMed
-
- Wasserman K, Zhang YY, Gitt A, Belardinelli R, Koike A, Lubarsky L, Agostoni PG.. Lung function and exercise gas exchange in chronic heart failure. Circulation 1997;96:2221–2227. - PubMed
-
- Thompson RB, Pagano JJ, Chow K, Sekowski V, Paterson I, Ezekowitz J, Anderson T, Dyck JRB, Haykowsky MJ.. Subclinical pulmonary edema is associated with reduced exercise capacity in HFpEF and HFrEF. J Am Coll Card 2017;70:1827–1828. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
