

Proximal pulmonary vascular stiffness as a prognostic factor in children with pulmonary arterial hypertension
- PMID: 29788051
- PMCID: PMC6343079
- DOI: 10.1093/ehjci/jey069
Proximal pulmonary vascular stiffness as a prognostic factor in children with pulmonary arterial hypertension
Abstract
Aims: Main pulmonary artery (MPA) stiffness and abnormal flow haemodynamics in pulmonary arterial hypertension (PAH) are strongly associated with elevated right ventricular (RV) afterload and associated with disease severity and poor clinical outcomes in adults with PAH. However, the long-term effects of MPA stiffness on RV function in children with PAH remain poorly understood. This study is the first comprehensive evaluation of MPA stiffness in children with PAH, delineating the mechanistic relationship between flow haemodynamics and MPA stiffness as well as the prognostic ability of these measures regarding clinical outcomes.
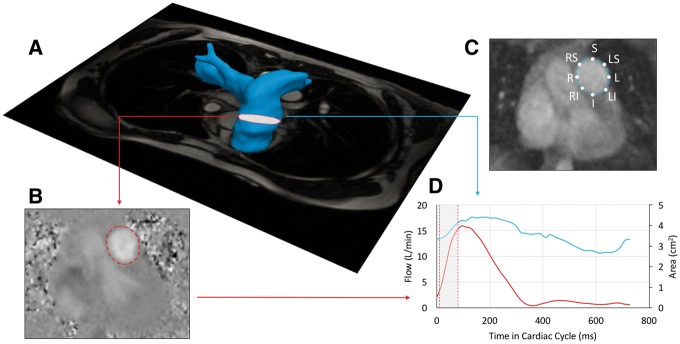
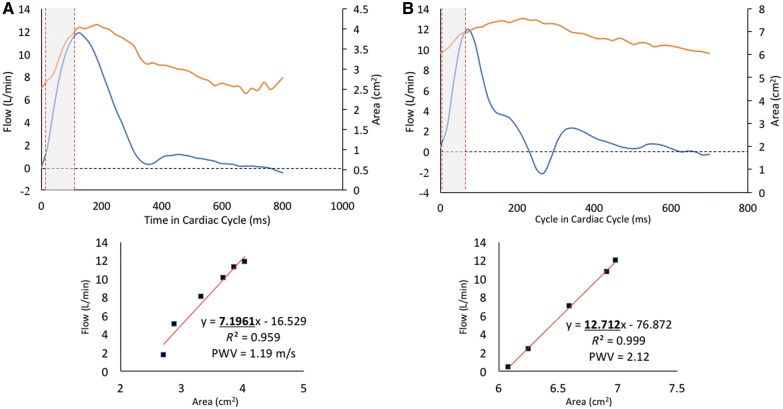
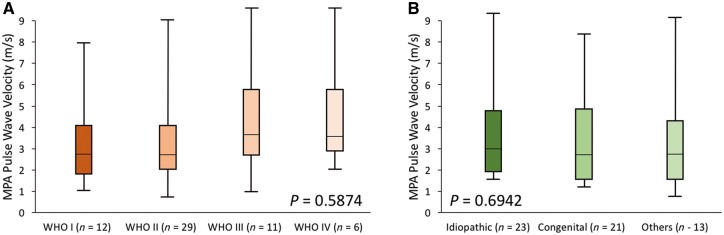
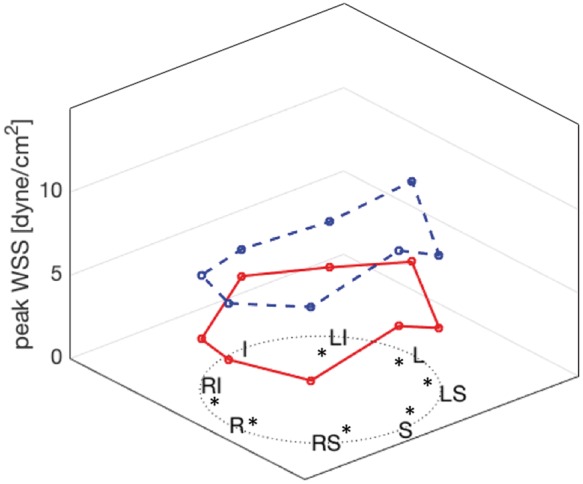
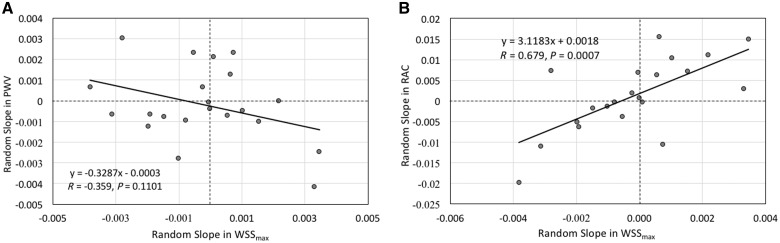
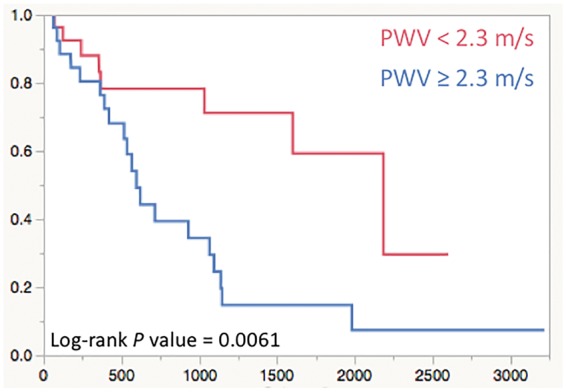
Methods and results: Fifty-six children diagnosed with PAH underwent baseline cardiac magnetic resonance (CMR) acquisition and were compared with 23 control subjects. MPA stiffness and wall shear stress (WSS) were evaluated using phase contrast CMR and were evaluated for prognostic potential along with standard RV volumetric and functional indices. Pulse wave velocity (PWV) was significantly increased (2.8 m/s vs. 1.4 m/s, P < 0.0001) and relative area change (RAC) was decreased (25% vs. 37%, P < 0.0001) in the PAH group, correlating with metrics of RV performance. Decreased WSS was associated with a decrease in RAC over time (r = 0.679, P < 0.001). For each unit increase in PWV, there was approximately a 3.2-fold increase in having a moderate clinical event.
Conclusion: MPA stiffness assessed by non-invasive CMR was increased in children with PAH and correlated with RV performance, suggesting that MPA stiffness is a major contribution to RV dysfunction. PWV is predictive of moderate clinical outcomes, and may be a useful prognostic marker of disease activity in children with PAH.
Figures
References
-
- Tozzi CA, Christiansen DL, Poiani GJ, Riley DJ.. Excess collagen in hypertensive pulmonary arteries decreases vascular distensibility. Am J Respir Crit Care Med 1994;149:1317–26. - PubMed
-
- Stenmark KR, Fagan KA, Frid MG.. Hypoxia-induced pulmonary vascular remodeling: cellular and molecular mechanisms. Circ Res 2006;99:675–91. - PubMed
-
- Abman SH, Hansmann G, Archer SL, Ivy DD, Adatia I, Chung WK. et al. Pediatric pulmonary hypertension. Circulation 2015;132:2037–99. - PubMed
-
- Schäfer M, Myers C, Brown RD, Frid MG, Tan W, Hunter K. et al. Pulmonary arterial stiffness: toward a new paradigm in pulmonary arterial hypertension pathophysiology and assessment. Curr Hypertens Rep 2016;18:4. - PubMed
-
- Reiter G, Reiter U, Kovacs G, Kainz B, Schmidt K, Maier R. et al. Magnetic resonance-derived 3-dimensional blood flow patterns in the main pulmonary artery as a marker of pulmonary hypertension and a measure of elevated mean pulmonary arterial pressure. Circ Cardiovasc Imaging 2008;1:23–30. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
