

Systematic review and meta-analysis of the evidence for oral nutritional intervention on nutritional and clinical outcomes during chemo(radio)therapy: current evidence and guidance for design of future trials
- PMID: 29788170
- PMCID: PMC5961292
- DOI: 10.1093/annonc/mdy114
Systematic review and meta-analysis of the evidence for oral nutritional intervention on nutritional and clinical outcomes during chemo(radio)therapy: current evidence and guidance for design of future trials
Abstract
Background: Driven by reduced nutritional intakes and metabolic alterations, malnutrition in cancer patients adversely affects quality of life, treatment tolerance and survival. We examined evidence for oral nutritional interventions during chemo(radio)therapy.
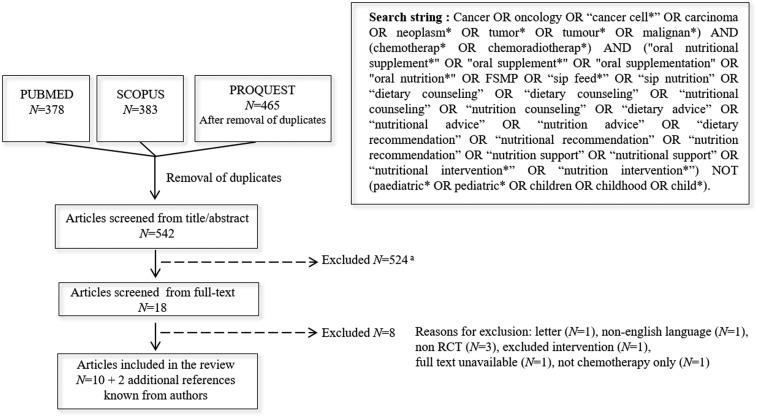
Design: We carried out a systematic review of randomized controlled trials (RCT) with either dietary counseling (DC), high-energy oral nutritional supplements (ONS) aiming at improving intakes or ONS enriched with protein and n-3 polyunsaturated fatty acids (PUFA) additionally aiming for modulation of cancer-related metabolic alterations. Meta-analyses were carried out on body weight (BW) response to nutritional interventions, with subgroup analyses for DC and/or high-energy ONS or high-protein n-3 PUFA-enriched ONS.
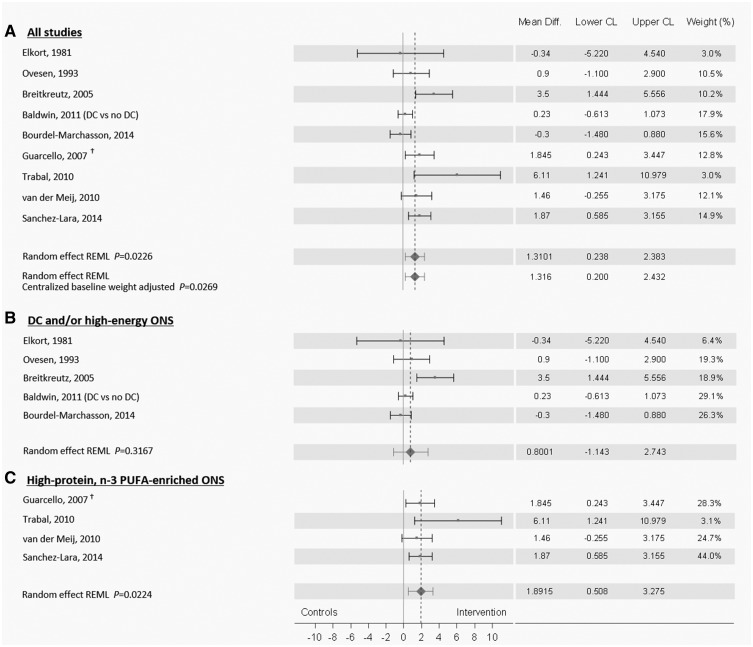
Results: Eleven studies were identified. Meta-analysis showed overall benefit of interventions on BW during chemo(radio)therapy (+1.31 kg, 95% CI 0.24-2.38, P = 0.02, heterogeneity Q = 21.1, P = 0.007). Subgroup analysis showed no effect of DC and/or high-energy ONS (+0.80 kg, 95% CI -1.14 to 2.74, P = 0.32; Q = 10.5, P = 0.03), possibly due to limited compliance and intakes falling short of intake goals. A significant effect was observed for high-protein n-3 PUFA-enriched intervention compared with isocaloric controls (+1.89 kg, 95% CI 0.51-3.27, P = 0.02; Q = 3.1 P = 0.37). High-protein, n-3 PUFA-enriched ONS studies showed attenuation of lean body mass loss (N = 2 studies) and improvement of some quality of life domains (N = 3 studies). Overall, studies were limited in number, heterogeneous, and inadequately powered to show effects on treatment toxicity or survival.
Conclusion: This systematic review suggests an overall positive effect of nutritional interventions during chemo(radio)therapy on BW. Subgroup analyses showed effects were driven by high-protein n-3 PUFA-enriched ONS, suggesting the benefit of targeting metabolic alterations. DC and/or high-energy ONS were less effective, likely due to cumulative caloric deficits despite interventions. We highlight the need and provide recommendations for well-designed RCT to determine the effect of nutritional interventions on clinical outcomes, with specific focus on reaching nutritional goals and providing the right nutrients, as part of an integral supportive care approach.
Figures
Comment in
-
It is time to rethink weight loss in cancer.Ann Oncol. 2018 May 1;29(5):1090-1091. doi: 10.1093/annonc/mdy112. Ann Oncol. 2018. PMID: 29788171 No abstract available.
References
-
- Nitenberg G, Raynard B.. Nutritional support of the cancer patient: issues and dilemmas. Crit Rev Oncol/Hematol 2000; 34(3): 137–168. - PubMed
-
- Laviano A, Meguid MM.. Nutritional issues in cancer management. Nutrition 1996; 12(5): 358–371. - PubMed
-
- Hébuterne X, Lemarié E, Michallet M. et al. Prevalence of malnutrition and current use of nutrition support in patients with cancer. JPEN J Parenter Enteral Nutr 2014; 38(2): 196–204. - PubMed
-
- Gyan E, Raynard B, Durand JP. et al. Malnutrition in patients with cancer. JPEN J Parenter Enteral Nutr 2017; 148607116688881 - PubMed
-
- Van Cutsem E, Arends J.. The causes and consequences of cancer-associated malnutrition. Eur J Oncol Nurs 2005; 9: S51–S63. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
