

Feasibility and effectiveness of laparoscopic transgastric stapler-assisted circumferential esophageal mucosectomy and simultaneous fundoplication in a pig model
- PMID: 29788275
- PMCID: PMC6124652
- DOI: 10.1093/dote/doy030
Feasibility and effectiveness of laparoscopic transgastric stapler-assisted circumferential esophageal mucosectomy and simultaneous fundoplication in a pig model
Abstract
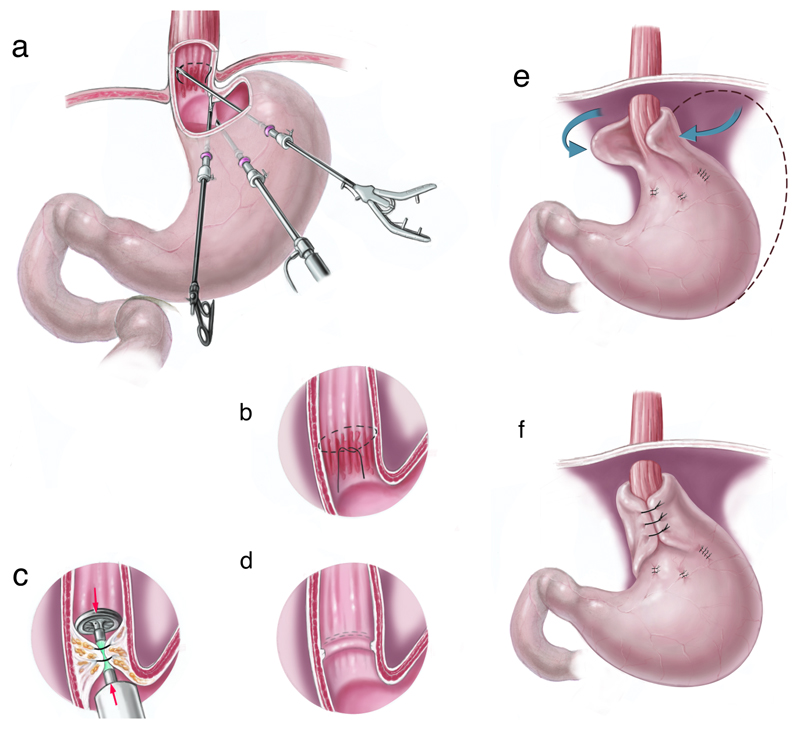
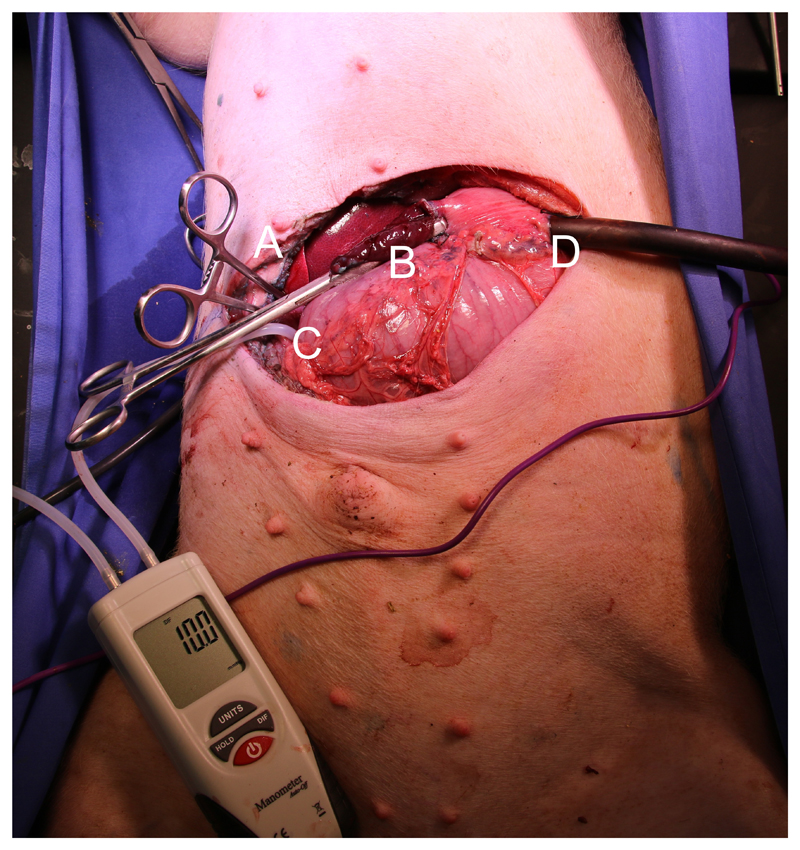
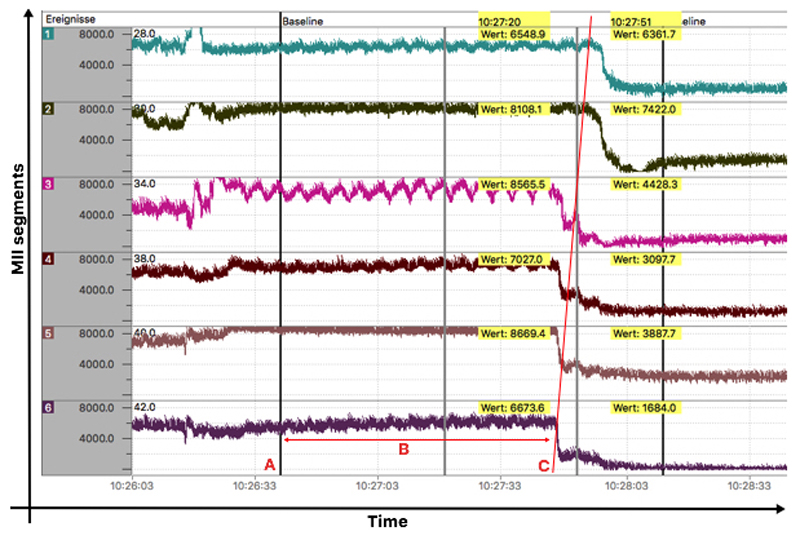
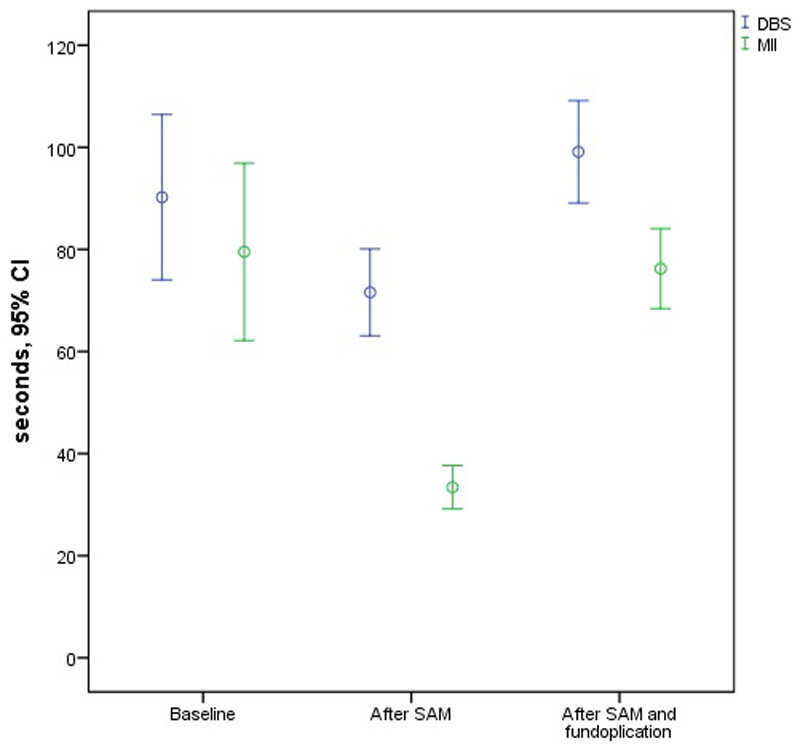
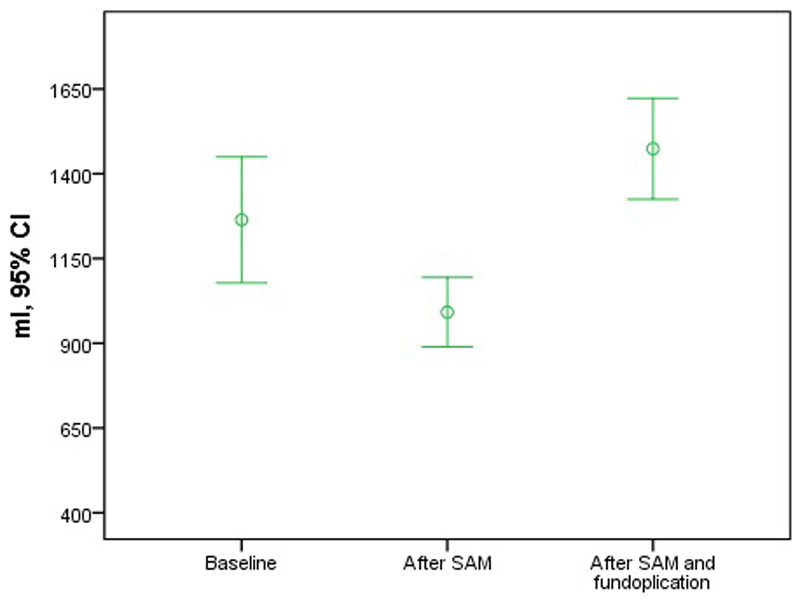
Laparoscopic transgastric stapler-assisted mucosectomy (SAM) has been described for minimally invasive circumferential en bloc resection of Barrett's esophagus (BE). Conceivably long-term disease control might be achieved by adding antireflux surgery after resection of BE by SAM. The aim of this study was to assess the feasibility of combined SAM and fundoplication in one laparoscopic procedure in six pigs. Furthermore, the competence of the gastroesophageal junction (GEJ) was assessed at baseline, after SAM, and after subsequent laparoscopic fundoplication. At each measuring point reflux measurements were repeated 6 times in each pig. Blue-colored water was infused into the stomach to provoke reflux. Intragastric yield pressure and volume were recorded until drainage of blue solution (DBS) was noted. Time to reflux was measured by DBS and by multichannel intraluminal impedance (MII). In all animals SAM followed by laparoscopic fundoplication was feasible in a single session. A weakening of the GEJ was found after SAM, indicated by decreased yield pressure (11.5 mmHg vs. 8.5 mmHg; P < 0.001), time to DBS (90 seconds vs. 60 seconds; P = 0.008) and MII (80 seconds vs. 33 seconds; P < 0.001). After additional Nissen fundoplication the GEJ competence was restored, with measurements returning to baseline values (time to DBS 99 seconds; P = 0.15; MII 76 seconds; P = 0.84). The yield pressure increased from 11.5 mmHg at baseline to 19.7 mmHg after SAM and fundoplication (P < 0.001). Laparoscopic fundoplication and SAM may be combined in a single laparoscopic session. Although the GEJ was weakened after SAM, Nissen fundoplication restored the GEJ as an effective reflux barrier in this experiment. For clinical validation, the results need to be confirmed in a prospective human trial.
Conflict of interest statement
Daniel C. Steinemann is supported by the Swiss National Science Foundation (Grant P300PB-161099/1) and the Margarete and Walter Lichtenstein Foundation, Basel, Switzerland (DMS2321). All other authors have nothing to disclose.
Figures


Similar articles
-
The relationship between gastroesophageal junction integrity and symptomatic fundoplication outcomes.Surg Endosc. 2020 Mar;34(3):1387-1392. doi: 10.1007/s00464-019-06921-9. Epub 2019 Jun 18. Surg Endosc. 2020. PMID: 31214803
-
[Comparison of surgical patients with gastroesophageal reflux disease and Barrett's esophagus].Magy Seb. 2014 Oct;67(5):287-96. doi: 10.1556/MaSeb.67.2014.5.1. Magy Seb. 2014. PMID: 25327403 Hungarian.
-
The laparoscopic Nissen-Hill hybrid: pilot study of a combined antireflux procedure.Surg Endosc. 2013 Jun;27(6):1945-52. doi: 10.1007/s00464-012-2692-7. Epub 2013 Jan 10. Surg Endosc. 2013. PMID: 23306589 Clinical Trial.
-
Impedance planimetry (EndoFLIP™) reveals changes in gastroesophageal junction compliance during fundoplication.Surg Endosc. 2022 Sep;36(9):6801-6808. doi: 10.1007/s00464-021-08966-1. Epub 2022 Jan 11. Surg Endosc. 2022. PMID: 35015103 Review.
-
[Minimally invasive surgery for gastroesophageal reflux disease].Korean J Gastroenterol. 2007 Oct;50(4):220-5. Korean J Gastroenterol. 2007. PMID: 18159185 Review. Korean.
References
-
- Lagergren J, Bergstrom R, Lindgren A, et al. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999;340(11):825–31. - PubMed
-
- Ireland CJ, Fielder AL, Thompson SK, et al. Development of a risk prediction model for Barrett's esophagus in an Australian population. Dis Esophagus. 2017;30(11):1–8. - PubMed
-
- Duits LC, Phoa KN, Curvers WL, et al. Barrett's oesophagus patients with low-grade dysplasia can be accurately risk-stratified after histological review by an expert pathology panel. Gut. 2015;64(5):700–6. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
