

Comparison of Clostridioides difficile Stool Toxin Concentrations in Adults With Symptomatic Infection and Asymptomatic Carriage Using an Ultrasensitive Quantitative Immunoassay
- PMID: 29788296
- PMCID: PMC6293008
- DOI: 10.1093/cid/ciy415
Comparison of Clostridioides difficile Stool Toxin Concentrations in Adults With Symptomatic Infection and Asymptomatic Carriage Using an Ultrasensitive Quantitative Immunoassay
Abstract
Background: We used an ultrasensitive, quantitative single molecule array (Simoa) immunoassay to test whether concentrations of Clostridioides (formerly Clostridium) difficile toxins A and/or B in the stool of adult inpatients with C. difficile infection (CDI) were higher than in asymptomatic carriers of toxinogenic C. difficile.
Methods: Patients enrolled as CDI-NAAT had clinically significant diarrhea and a positive nucleic acid amplification test (NAAT), per US guidelines, and received CDI treatment. Potential carriers had recently received antibiotics and did not have diarrhea; positive NAAT confirmed carriage. Baseline stool samples were tested by Simoa for toxin A and B.
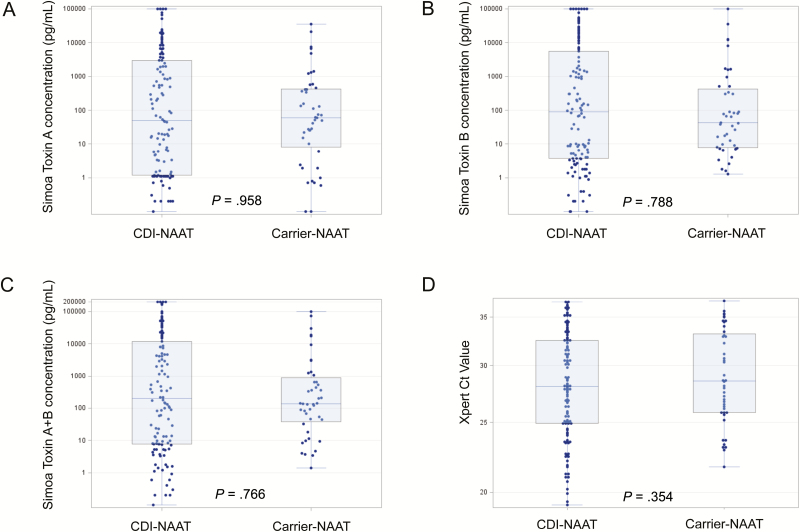
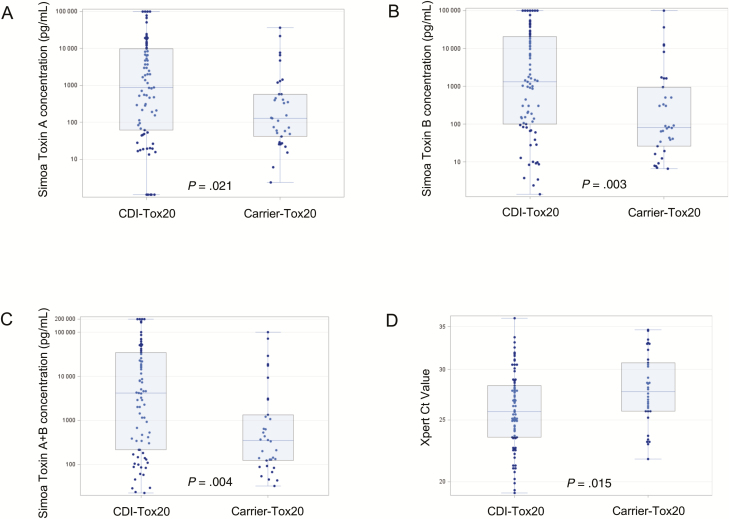
Results: Stool toxin concentrations in both CDI-NAAT (n = 122) and carrier-NAAT (n = 44) cohorts spanned 5 logs (0 pg/mL to >100000 pg/mL). Seventy-nine of 122 (65%) CDI-NAAT and 34 of 44 (77%) carrier-NAAT had toxin A + B concentration ≥20 pg/mL (clinical cutoff). Median toxin A, toxin B, toxin A + B, and NAAT cycle threshold (Ct) values in CDI-NAAT and carrier-NAAT cohorts were similar (toxin A, 50.6 vs 60.0 pg/mL, P = .958; toxin B, 89.5 vs 42.3 pg/mL, P = .788; toxin A + B, 197.2 vs 137.3 pg/mL, P = .766; Ct, 28.1 vs 28.6, P = .354). However, when CDI/carrier cohorts were limited to those with detectable toxin, respective medians were significantly different (A: 874.0 vs 129.7, P = .021; B: 1317.0 vs 81.7, P = .003, A + B, 4180.7 vs 349.6, P = .004; Ct, 25.8 vs 27.7, P = .015).
Conclusions: Toxin concentration did not differentiate an individual with CDI from one with asymptomatic carriage. Median stool toxin concentrations in groups with CDI vs carriage differed, but only when groups were defined by detectable stool toxin (vs positive NAAT).
Figures
Comment in
-
Frequency of Positive Enzyme Immunoassay for Toxin in Stool of Asymptomatic Carriers of Clostridium difficile.Clin Infect Dis. 2019 Feb 1;68(4):711. doi: 10.1093/cid/ciy701. Clin Infect Dis. 2019. PMID: 30137260 No abstract available.
References
-
- McDonald LC, Gerding DN, Johnson S, et al. . Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis 2018; 66:987–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
