

Association between troponin-I levels and outcome in critically ill patients admitted to non-cardiac intensive care unit with high prevalence of cardiovascular risk factors
- PMID: 29788912
- PMCID: PMC5964705
- DOI: 10.1186/s12871-018-0515-7
Association between troponin-I levels and outcome in critically ill patients admitted to non-cardiac intensive care unit with high prevalence of cardiovascular risk factors
Abstract
Background: The association of troponin-I levels and outcome in medical-surgical ICU patients has been studied before in populations with low to moderate prevalence of cardiovascular risk factors. The objective in this article is to examine the association of troponin-I levels with hospital mortality in patients with high prevalence of cardiovascular risk factors who were admitted with medical-surgical indications to a non-cardiac intensive care unit.
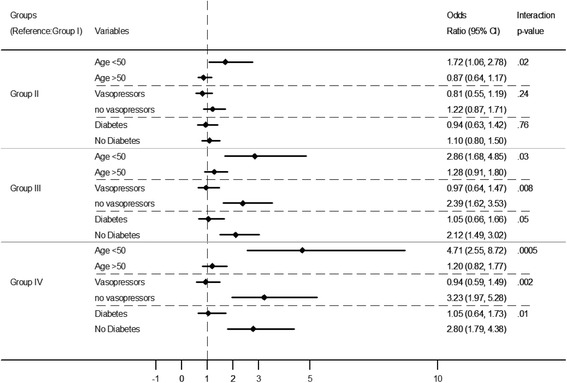
Methods: This was a retrospective study of adult patients admitted to a tertiary medical-surgical ICU between July 2001 and November 2011. Data were extracted from prospectively collected ICU and clinical laboratory databases. Patients were stratified based on the highest troponin-I level in the first 72 h of admission into four groups (Group I < 0.03, Group II = 0.03-0.3, Group III = 0.3-3 and Group IV > 3 ng/mL). Hospital mortality was the primary outcome. To study the association between elevated troponin-I and hospital mortality, we carried out multivariate logistic regression analyses with Group I as a reference group.
Results: During the study period, 3368 patients had troponin-I levels measured in the first 72 h, of whom 1293 (38.3%) were diabetic and 1356 (40.2%) were chronically hypertensive. Among the study population, 2719 (81%) had elevated troponin-I levels (0.03 ng/mL and higher). Hospital mortality increased steadily as the troponin-I levels increased. Hospital mortality was 23.4% for Group I, 33.2% for Group II (adjusted odds ratio (aOR) 1.08, 95% confidence interval (CI) 0.84, 1.38), 49.6% for Group III (aOR = 1.64, 95% CI 1.24, 2.17), and 57.4% for Group IV (aOR 1.80, 95% CI 1.30, 2.49). The association of increased mortality with increased troponin level was observed whether patients had underlying advanced heart failure or not. Subgroup analysis showed an increased mortality in patients aged < 50 years, non-diabetics and not on vasopressors.
Conclusion: In a population with high prevalence of diabetes and hypertension, elevated troponin-I was frequently observed in medical-surgical critically ill patients, and showed a level-dependent association with hospital mortality.
Keywords: Critical care; ICU; Mortality; Troponin-I.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the National Guard Health Affairs Institutional Review Board, Riyadh, Saudi Arabia with the approval number RR11/137 and conducted in accordance with the amended Declaration of Helsinki.
This was a retrospective study of adult patients admitted to an ICU of a tertiary care center in Riyadh, Saudi Arabia from July 2001 to November 2011. Data were extracted from prospectively collected ICU and clinical laboratory databases. Informed consent was waived by the IRB because of the observational nature of the study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Elevated troponin and myocardial infarction in the intensive care unit: a prospective study.Crit Care. 2005;9(6):R636-44. doi: 10.1186/cc3816. Epub 2005 Sep 28. Crit Care. 2005. PMID: 16280062 Free PMC article.
-
Association between statin therapy and outcomes in critically ill patients: a nested cohort study.BMC Clin Pharmacol. 2011 Aug 6;11:12. doi: 10.1186/1472-6904-11-12. BMC Clin Pharmacol. 2011. PMID: 21819615 Free PMC article. Clinical Trial.
-
Association Between Dexamethasone and Delirium in Critically Ill Patients: A Retrospective Cohort Study of a Large Clinical Database.J Surg Res. 2021 Jul;263:89-101. doi: 10.1016/j.jss.2021.01.027. Epub 2021 Feb 24. J Surg Res. 2021. PMID: 33639374
-
Elevated cardiac troponin measurements in critically ill patients.Arch Intern Med. 2006 Dec 11-25;166(22):2446-54. doi: 10.1001/archinte.166.22.2446. Arch Intern Med. 2006. PMID: 17159009 Review.
-
JOE DOUPE LECTURE: Cardiac troponin in the intensive care unit.Clin Invest Med. 2009 Oct 1;32(5):E405-10. doi: 10.25011/cim.v32i5.6929. Clin Invest Med. 2009. PMID: 19796582 Review.
Cited by
-
The Clinical Association between Carbon Monoxide Poisoning and Myocardial Injury as Measured by Elevated Troponin I Levels.J Clin Med. 2023 Aug 25;12(17):5529. doi: 10.3390/jcm12175529. J Clin Med. 2023. PMID: 37685595 Free PMC article.
-
Cardiac troponin I predicts clinical outcome of patients with cancer at emergency department.Clin Cardiol. 2020 Dec;43(12):1585-1591. doi: 10.1002/clc.23486. Epub 2020 Oct 21. Clin Cardiol. 2020. PMID: 33085130 Free PMC article.
-
Biochemical, electrolytic, and cardiovascular evaluations in cats with urethral obstruction.Vet World. 2021 Aug;14(8):2002-2008. doi: 10.14202/vetworld.2021.2002-2008. Epub 2021 Aug 4. Vet World. 2021. PMID: 34566314 Free PMC article.
-
Demand Ischemia as a Predictor of Mortality in Older Patients With Delirium.Front Cardiovasc Med. 2022 Jun 6;9:917252. doi: 10.3389/fcvm.2022.917252. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35734279 Free PMC article.
-
Markers of myocardial injury in the prediction of short-term COVID-19 prognosis.Rev Esp Cardiol (Engl Ed). 2021 Jul;74(7):576-583. doi: 10.1016/j.rec.2020.09.011. Epub 2020 Sep 29. Rev Esp Cardiol (Engl Ed). 2021. PMID: 33153955 Free PMC article.
References
-
- Alpert JS, Thygesen K, Antman E, et al. Myocardial infarction redefined--a consensus document of the joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959–969. doi: 10.1016/S0735-1097(00)00804-4. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
