

Blood Pressure-Attained Analysis of ATACH 2 Trial
- PMID: 29789395
- PMCID: PMC7224409
- DOI: 10.1161/STROKEAHA.117.019845
Blood Pressure-Attained Analysis of ATACH 2 Trial
Abstract
Background and purpose: We compared the rates of death or disability, defined by modified Rankin Scale score of 4 to 6, at 3 months in patients with intracerebral hemorrhage according to post-treatment systolic blood pressure (SBP)-attained status.
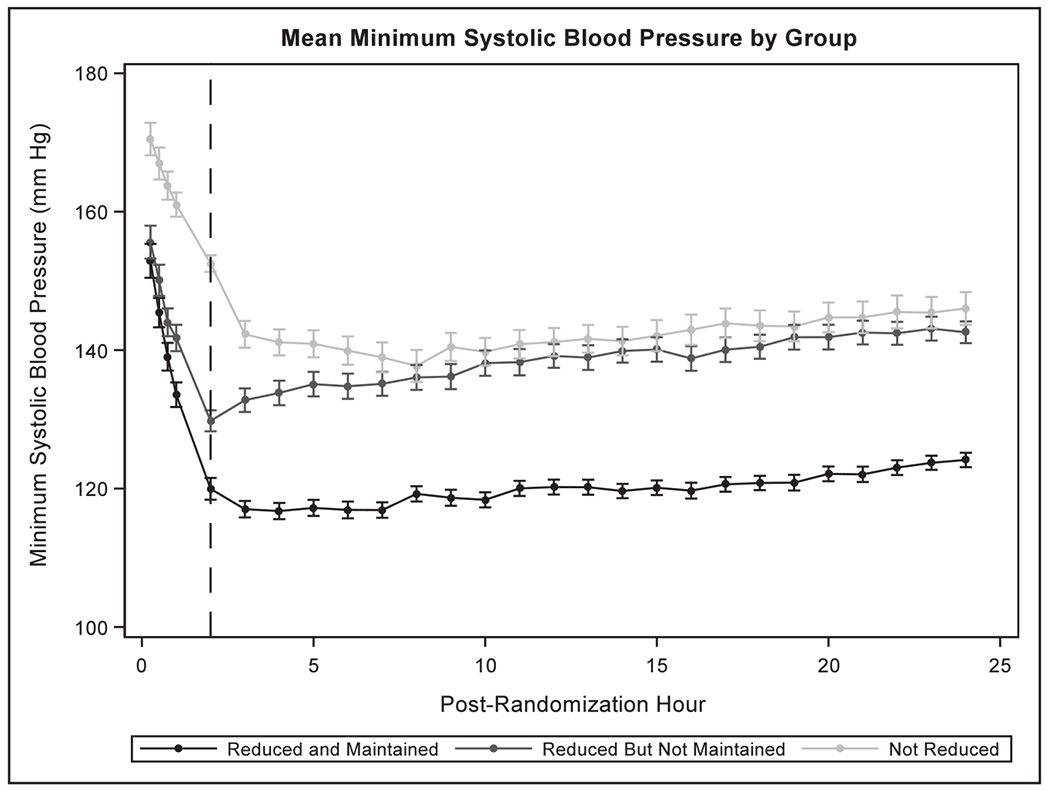
Methods: We divided 1000 subjects with SBP ≥180 mm Hg who were randomized within 4.5 hours of symptom onset as follows: SBP <140 mm Hg achieved or not achieved within 2 hours; subjects in whom SBP <140 mm Hg was achieved within 2 hours were further divided: SBP <140 mm Hg for 21 to 22 hours (reduced and maintained) or SBP was ≥140 mm Hg for at least 2 hours during the period between 2 and 24 hours (reduced but not maintained).
Results: Compared with subjects without reduction of SBP <140 mm Hg within 2 hours, subjects with reduction and maintenance of SBP <140 mm Hg within 2 hours had a similar rate of death or disability (relative risk of 0.98; 95% confidence interval, 0.74-1.29). The rates of neurological deterioration within 24 hours were significantly higher in reduced and maintained group (10.4%; relative risk, 1.98; 95% confidence interval, 1.08-3.62) and in reduced but not maintained group (11.5%; relative risk, 2.08; 95% confidence interval, 1.15-3.75) compared with reference group. The rates of cardiac-related adverse events within 7 days were higher among subjects with reduction and maintenance of SBP <140 mmHg compared to subjects without reduction (11.2% versus 6.4%).
Conclusions: No decline in death or disability but higher rates of neurological deterioration and cardiac-related adverse events were observed among intracerebral hemorrhage subjects with reduction with and without maintenance of intensive SBP goals.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT01176565.
Keywords: acute hypertensive response; blood pressure; cerebral hemorrhage; clinical trial; humans.
© 2018 American Heart Association, Inc.
Figures

References
-
- Qureshi AI, Palesch YY, Barsan WG, Hanley DF, Hsu CY, Martin RL, et al.; ATACH-2 Trial Investigators and the Neurological Emergency Treatment Trials Network. Intensive blood-pressure lowering in patients with acute cerebral hemorrhage. N Engl J Med. 2016;375:1033–1043. doi: 10.1056/NEJMoa1603460. - DOI - PMC - PubMed
-
- Qureshi AI, Hutson AD, Harbaugh RE, Stieg PE, Hopkins LN; North American Trial of Unruptured and Ruptured Aneurysms Planning Committee. Methods and design considerations for randomized clinical trials evaluating surgical or endovascular treatments for cerebrovascular diseases. Neurosurgery. 2004;54:248–264; discussion 264-247. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
