

The pharmacokinetics, pharmacodynamics and tolerability of PUR0200, a novel tiotropium formulation, in chronic obstructive pulmonary disease
- PMID: 29790581
- PMCID: PMC6089803
- DOI: 10.1111/bcp.13645
The pharmacokinetics, pharmacodynamics and tolerability of PUR0200, a novel tiotropium formulation, in chronic obstructive pulmonary disease
Abstract
Aims: PUR0200 is a tiotropium bromide formulation engineered with the iSPERSE dry powder delivery technology. PUR0200 is being developed as a bioequivalent alternative to tiotropium bromide, delivered using Spiriva® HandiHaler® (HH). We investigated the bronchodilator effects, pharmacokinetics and safety of PUR0200 in patients with chronic obstructive pulmonary disease (COPD).
Methods: This was a randomized, placebo-controlled, crossover study using different PUR0200 doses and the comparator tiotropium HH. In vitro aerodynamic particle size distribution (aPSD) characterization of PUR0200 and tiotropium HH are presented. The main endpoints included forced expiratory volume in 1 s (FEV1 ) trough and (0-24 h) and pharmacokinetic parameters.
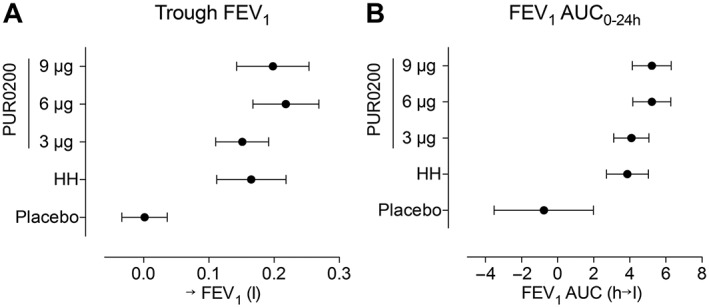
Results: The increased fine-particle fraction of PUR0200 demonstrated by testing using the next-generation impactor increased the proportion of drug available for lung deposition compared with the tiotropium HH. There was a numerical dose-response effect for PUR0200 on FEV1 , with 3 μg demonstrating a lower effect than higher doses. The placebo-adjusted mean (95% confidence interval) increases from baseline at 24 h postdose were 150 ml (100-200), 210 ml (160-270) and 200 ml (140-250) for 3 μg, 6 μg and 9 μg doses of PUR0200, respectively. Tiotropium HH (18 μg) caused a mean 169 ml (standard deviation 157ml) improvement in trough FEV1 , which was not significantly different to the PUR0200 effects at any of the tested doses.
Conclusions: PUR0200 treatment caused bronchodilation in COPD patients that was similar in magnitude to that caused by tiotropium HH. This enabled a similar clinical effect on lung function to be achieved with PUR0200 using a lower metered dose of tiotropium compared with tiotropium HH.
Keywords: COPD; FEV1; PUR0200; pharmacokinetics; tiotropium.
© 2018 The British Pharmacological Society.
Figures




References
-
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med 2017; 195: 557–582. - PubMed
-
- Singh D, Roche N, Halpin D, Agusti A, Wedzicha JA, Martinez FJ. Current controversies in the pharmacological treatment of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2016; 194: 541–549. - PubMed
-
- Tashkin DP, Celli B, Senn S, Burkhart D, Kesten S, Menjoge S, et al A 4‐year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med 2008; 359: 1543–1554. - PubMed
-
- Maesen FPV, Smeets JJ, Sledsens TJH, Wald FDM, Cornelissen PJG, on behalf of a Dutch study group . Tiotropium bromide, a new long‐acting bronchodilator: a pharmacodynamic study in patients with chronic obstructive pulmonary disease. Eur Respir J 1995; 8: 1506–1513. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
