

The Hospital Readmissions Reduction Program-learning from failure of a healthcare policy
- PMID: 29791084
- PMCID: PMC6105419
- DOI: 10.1002/ejhf.1212
The Hospital Readmissions Reduction Program-learning from failure of a healthcare policy
Abstract
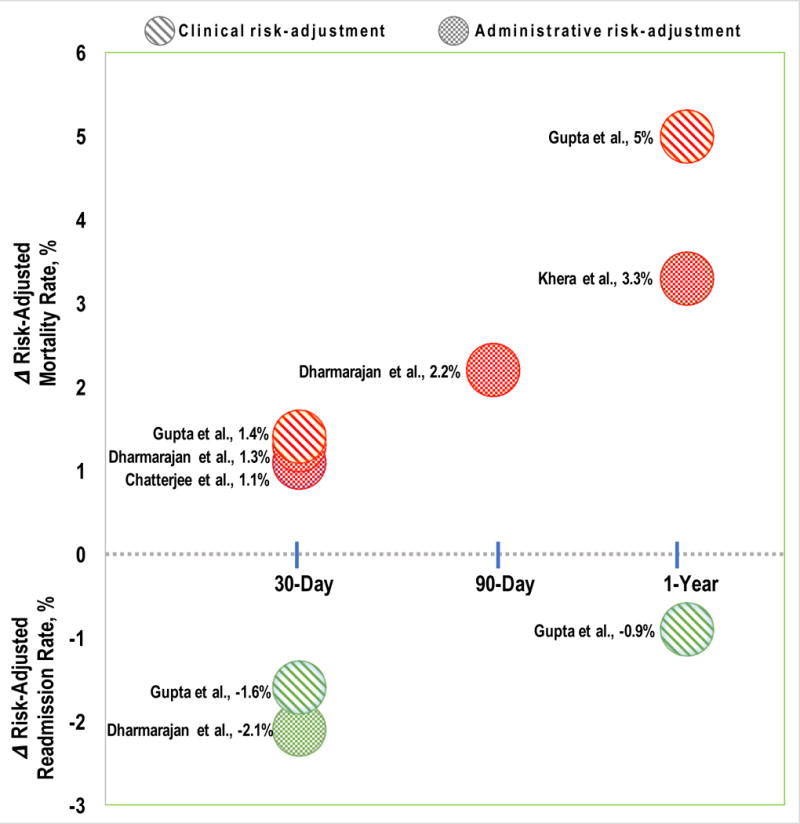
Heart failure is the leading cause of readmissions in patients aged ≥65 years with high associated societal and economic costs. The utilization metric of 30-day risk standardized readmission rates (RSRRs) has therefore become a target to reduce healthcare costs. In this review, we discuss in detail the implementation, effectiveness, and unintended consequences of the Hospital Readmissions Reduction Program (HRRP)-the major healthcare policy approach in the U.S. to reduce readmissions by financially penalizing hospitals with higher than average 30-day RSRRs. The HRRP was enacted by the Patient Protection and Affordable Care Act of 2010 (popularly known as 'Obamacare'). The public reporting of RSRRs began in June 2009 and the HRRP readmission penalties went into effect starting fiscal year 2013. The policy had limited success in achieving its primary objective of reducing readmissions as the achieved reduction in heart failure readmissions was much smaller (∼9%) than anticipated (∼25%) with some of the reduction in RSRRs attributable to the artifact of administrative upcoding post-HRRP rather than an actual decline in readmissions. From the time of passage of this law, there have been significant concerns regarding gaming of the system such as increase in observation stays, delaying readmissions beyond discharge day 30, and inappropriate triage strategies in emergency departments in order to achieve lower readmission rates to avoid penalties. A series of independent reports have now suggested that implementation of the HRRP was associated with an increase in 30-day, 90-day, and 1-year risk-adjusted heart failure mortality in the U.S. with reversal in decade long trend of declining heart failure mortality. We review the evidence behind effect of the HRRP on readmissions and mortality outcomes as well as discuss various lessons to be learned from the design, implementation, and consequences of this policy.
Keywords: Healthcare policy; Heart failure; Mortality; Readmission.
© 2018 The Authors. European Journal of Heart Failure © 2018 European Society of Cardiology.
Figures
References
-
- Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, Nodari S, Lam CSP, Sato N, Shah AN, Gheorghiade M. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol. 2014;63(12):1123–1133. - PubMed
-
- Zuckerman RB, Sheingold SH, Orav EJ, Ruhter J, Epstein AM. Readmissions, Observation, and the Hospital Readmissions Reduction Program. N Engl J Med. 2016;374(16):1543–51. - PubMed
-
- The Facts on Medicare Spending and Financing. 2017 https://wwwkfforg/medicare/issue-brief/the-facts-on-medicare-spending-an... Accessed January 15, 2018.
-
- DeVore AD, Hammill BG, Hardy NC, Eapen ZJ, Peterson ED, Hernandez AF. Has Public Reporting of Hospital Readmission Rates Affected Patient Outcomes?: Analysis of Medicare Claims Data. J Am Coll Cardiol. 2016;67(8):963–72. - PubMed
-
- Aiming for fewer hospital U-turns: The Medicare Hospital Readmissions Reduction Program. 2017 https://wwwkfforg/medicare/issue-brief/aiming-for-fewer-hospital-u-turns... Accessed January 15, 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
