

BRCA1/2 Mutations and Bevacizumab in the Neoadjuvant Treatment of Breast Cancer: Response and Prognosis Results in Patients With Triple-Negative Breast Cancer From the GeparQuinto Study
- PMID: 29791287
- PMCID: PMC6067803
- DOI: 10.1200/JCO.2017.77.2285
BRCA1/2 Mutations and Bevacizumab in the Neoadjuvant Treatment of Breast Cancer: Response and Prognosis Results in Patients With Triple-Negative Breast Cancer From the GeparQuinto Study
Abstract
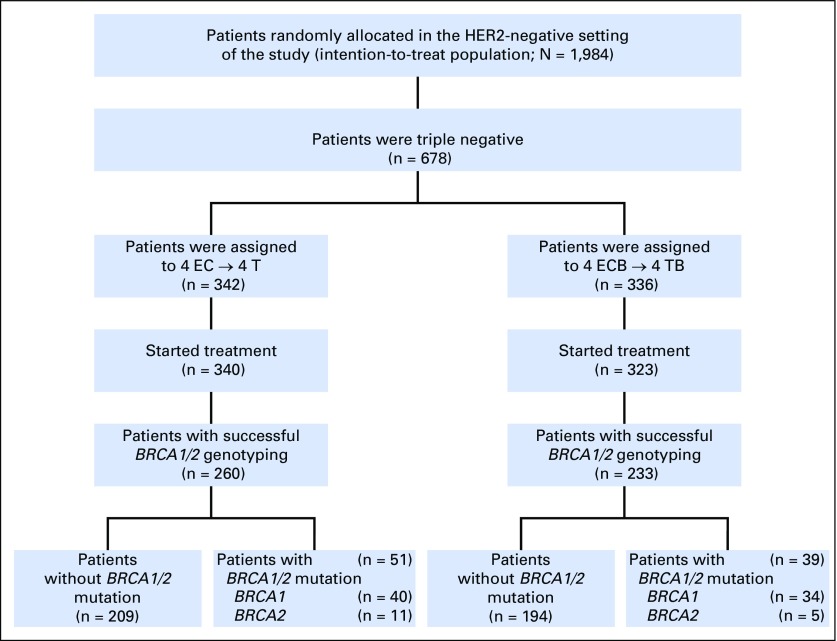
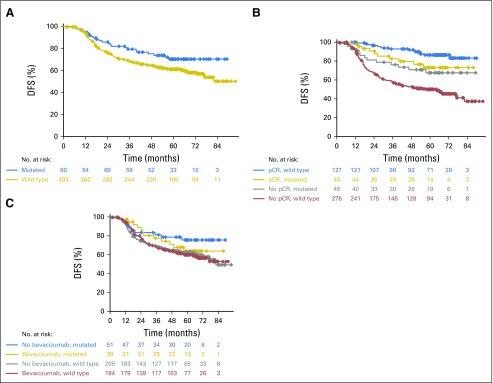
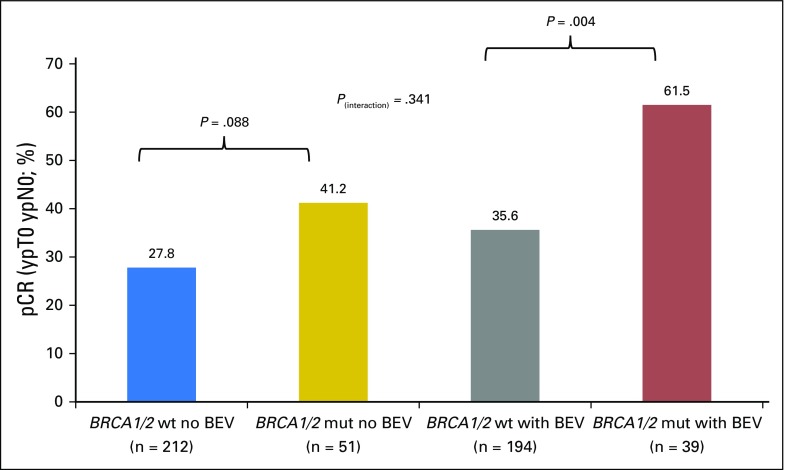
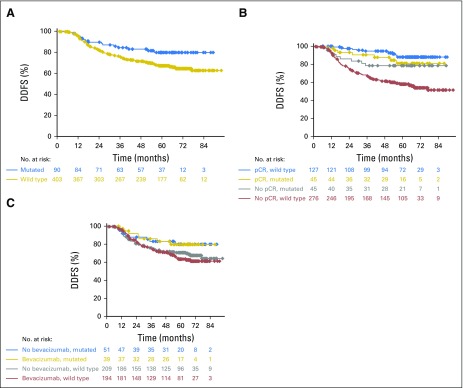
Purpose BRCA1/2 mutations are frequent in patients with triple-negative breast cancer (TNBC). These patients are often treated with primary systemic chemotherapy. The aim of this study was to analyze the effects of BRCA1/2 mutations on pathologic complete response (pCR) and disease-free survival (DFS) in a cohort of patients with TNBC treated with anthracycline and taxane-containing chemotherapy, with or without bevacizumab. Patients and Methods Germline DNA was sequenced to identify mutations in BRCA1 and BRCA2 in 493 patients with TNBC from the GeparQuinto study. The pCR rates were compared in patients with and without mutation, as well as in patients treated with and without bevacizumab. In addition, the influence of BRCA1/2 mutation status and pCR status on DFS was evaluated relative to treatment. Results BRCA1/2 mutations were detected in 18.3% of patients with TNBC. Overall, patients with mutations had a pCR rate of 50%, compared with 31.5% in patients without a mutation (odds ratio [OR], 2.17; 95% CI, 1.37 to 3.46; P = .001). The pCR rate among patients treated with bevacizumab was 61.5% for BRCA1/2 mutation carriers and 35.6% for those without mutations (OR, 2.90; 95% CI, 1.43 to 5.89; P = .004). pCR was a strong predictor of DFS for patients without BRCA1/2 mutations (hazard ratio, 0.18; 95% CI, 0.11 to 0.31) but not for patients with BRCA1/2 mutations (hazard ratio, 0.74; 95% CI, 0.32 to 1.69). Conclusion The addition of bevacizumab may increase the pCR after standard neoadjuvant chemotherapy for patients with TNBC with BRCA1/2 mutations. In patients treated with anthracycline and taxane-based chemotherapy (with or without bevacizumab), pCR was a weaker predictor of DFS for BRCA1/2 mutation carriers than for patients without mutations.
Trial registration: ClinicalTrials.gov NCT00567554.
Figures
Comment in
-
A new paradox for pCR in BRCA mutation carriers.Transl Cancer Res. 2019 Mar;8(Suppl 2):S99-S102. doi: 10.21037/tcr.2018.10.25. Transl Cancer Res. 2019. PMID: 35117073 Free PMC article. No abstract available.
References
-
- Cortazar P, Zhang L, Untch M, et al. : Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 384:164-172, 2014 - PubMed
-
- von Minckwitz G, Untch M, Blohmer JU, et al. : Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol 30:1796-1804, 2012 - PubMed
-
- Wang C, Zhang J, Wang Y, et al. : Prevalence of BRCA1 mutations and responses to neoadjuvant chemotherapy among BRCA1 carriers and non-carriers with triple-negative breast cancer. Ann Oncol 26:523-528, 2015 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
