

Screening for congenital fetal anomalies in low risk pregnancy: the Kenyatta National Hospital experience
- PMID: 29792180
- PMCID: PMC5966855
- DOI: 10.1186/s12884-018-1824-z
Screening for congenital fetal anomalies in low risk pregnancy: the Kenyatta National Hospital experience
Abstract
Background: Congenital malformations contribute significantly to the disease burden among children globally. A study conducted in Kenya on understanding the burden of surgical congenital anomalies, highlights the need for Kenyan health systems to go beyond the medical dimensions of illness. This could be achieved by linking knowledge of the severe congenital anomalies (CAs) and their impact of varying disability to the delivery of local health services and public health program planning. Subsequently, early detection of these congenital anomalies is vital and can be achieved through fetal ultrasonography. Studies have proven that antenatal ultrasound can successfully diagnose fetal abnormalities in many cases and therefore aid in counseling of parents and planning for early intervention. Although there are studies on screening of congenital anomalies in various populations, very few have been done in the African population and none to the best of our knowledge has been done in Kenya.
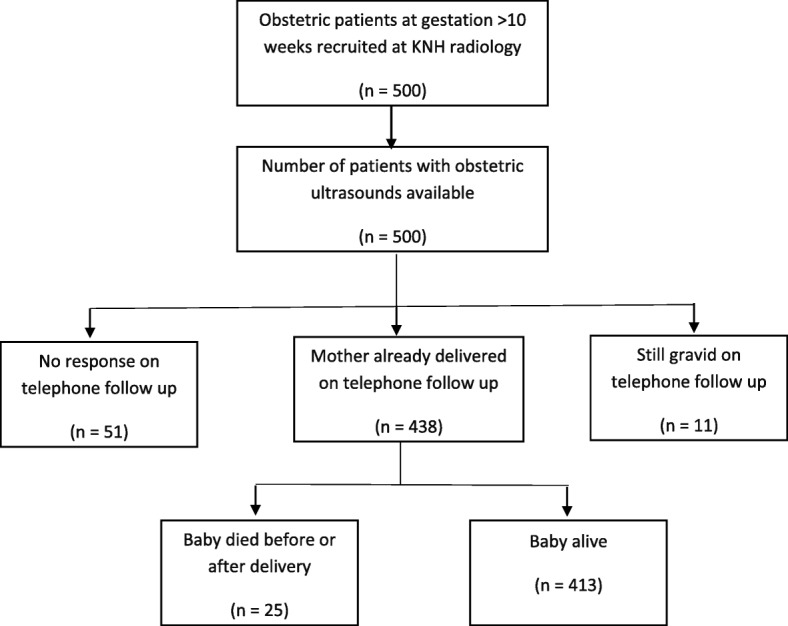
Methods: The patients, who underwent routine obstetric ultrasounds, were recruited into the study. The study population comprised patients who were referred from the obstetric clinic, casualty and other clinics within the hospital vicinity. Data of antenatal ultrasounds was statistically analyzed on structured data collection form to determine the prevalence of congenital anomalies.
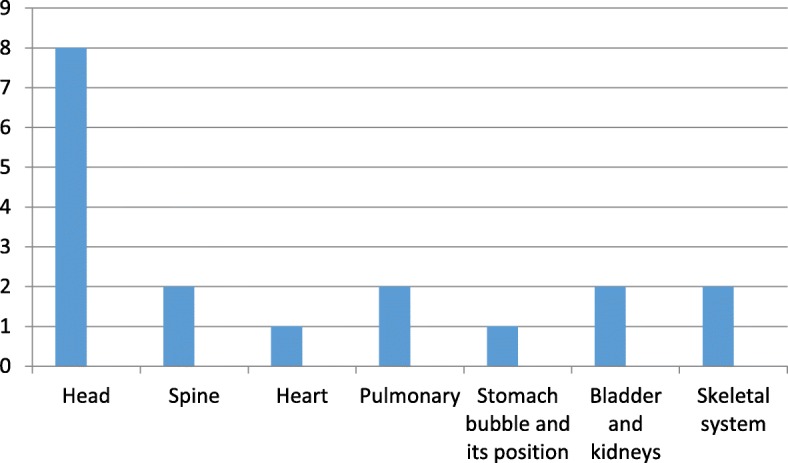
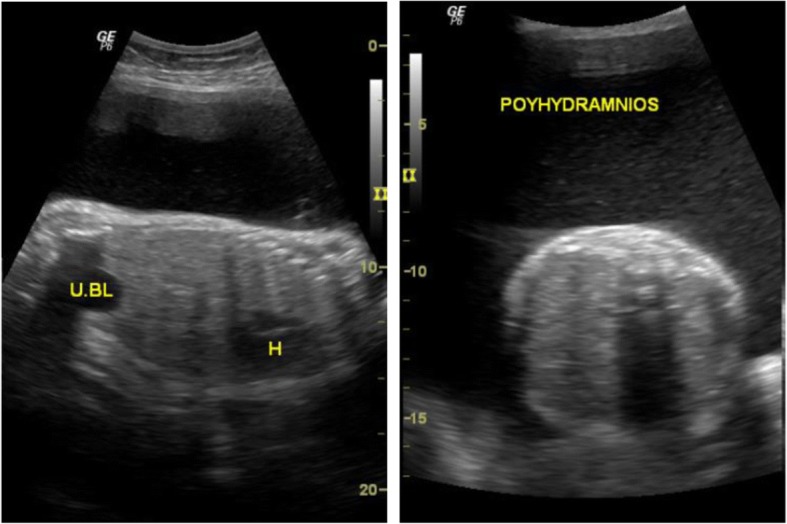
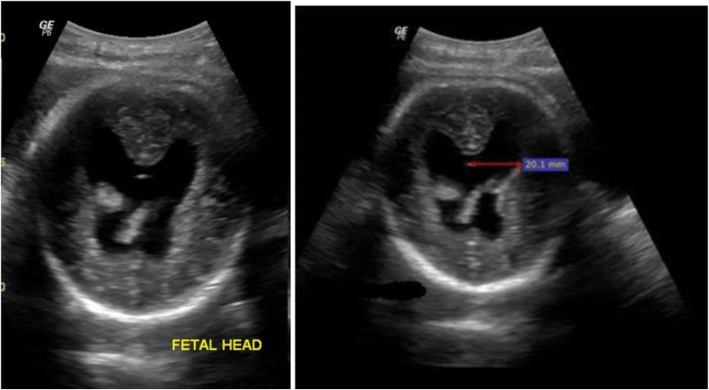
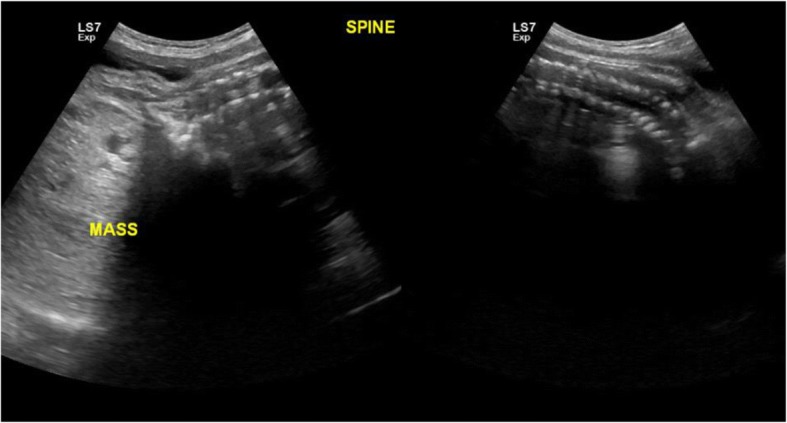
Results: Fifteen fetal anomalies were diagnosed in 500 women who came for routine ultrasound (3%). The mean age of the mothers was 28.2 years (SD ± 4.5) with an age range from 15 to 44 years. 400 (80%) of the mothers were aged between 27 and 34 years. The most frequently observed fetal anomalies involved the head (8/ 500; 1.6%). Each of the remaining anomalies affected less than 1% of the fetuses and included anomalies of the spine (2/ 500; 0.4%), pulmonary (2/ 500; 0.4%), renal and urinary tract (2/ 500; 0.4%) and skeletal systems (2/ 500; 0.4%). Majority, 9 of 15 (60%) of the fetuses with anomalies detected on prenatal ultrasound resulted in postnatal mortality within days of delivery.
Conclusion: Congenital anomalies prevalence in our setting compares with those found in other studies. From this study, major birth defects are a major cause of perinatal mortality.
Keywords: Low risk; Malformations; Obstetric; Sonography.
Conflict of interest statement
Ethics approval and consent to participate
Permission for the study was obtained from the Kenyatta National Hospital/University of Nairobi ethics and review committee, P699/11/2014.
Written informed consent was obtained from the study participants prior to their participation in the study.
Consent for publication
Verbal informed consent for publication was also obtained from the study participants during the study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Congenital anomalies fact sheet. WHO, 2015.
-
- Congenital PAV. Anomalies in rural black south African neonates--a silent epidemic? S Afr Med J. 1995;85(1):15–20. - PubMed
-
- MSaPJ MRO. Congenital malformations among newborns in Kenya. Afr J Food Agric Nutr Dev. 2009;9(3)
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
