

Effect of postoperative goal-directed therapy in cancer patients undergoing high-risk surgery: a randomized clinical trial and meta-analysis
- PMID: 29792232
- PMCID: PMC5964647
- DOI: 10.1186/s13054-018-2055-4
Effect of postoperative goal-directed therapy in cancer patients undergoing high-risk surgery: a randomized clinical trial and meta-analysis
Abstract
Background: Perioperative goal-directed hemodynamic therapy (GDHT) has been advocated in high-risk patients undergoing noncardiac surgery to reduce postoperative morbidity and mortality. We hypothesized that using cardiac index (CI)-guided GDHT in the postoperative period for patients undergoing high-risk surgery for cancer treatment would reduce 30-day mortality and postoperative complications.
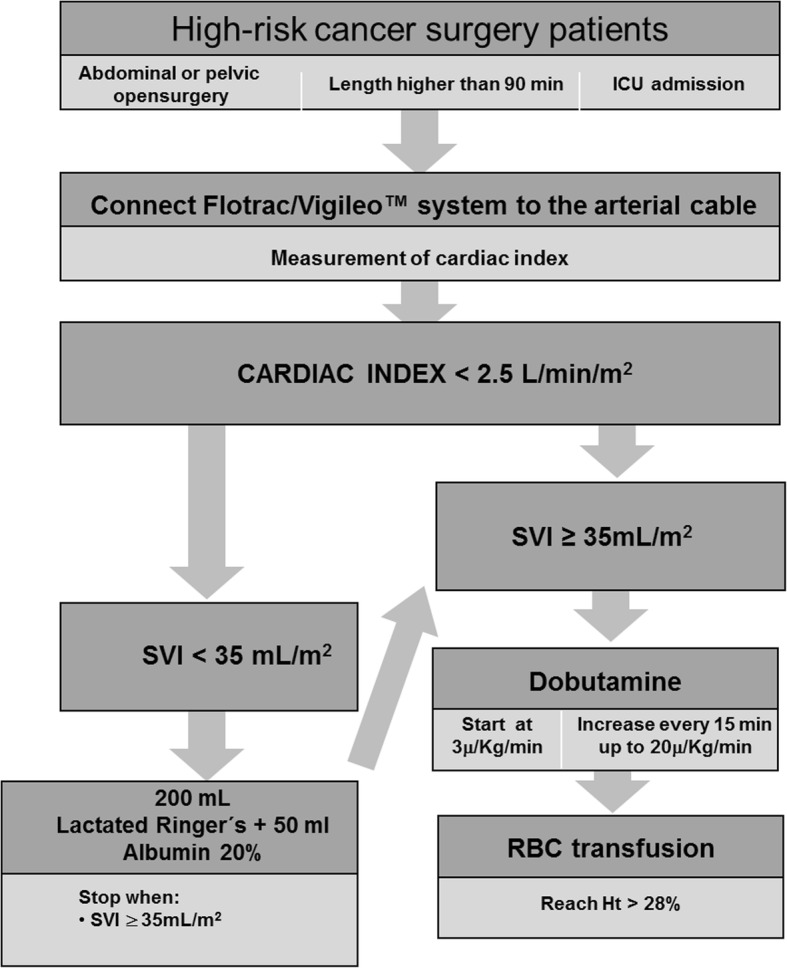
Methods: A randomized, parallel-group, superiority trial was performed in a tertiary oncology hospital. All adult patients undergoing high-risk cancer surgery who required intensive care unit admission were randomly allocated to a CI-guided GDHT group or to a usual care group. In the GDHT group, postoperative therapy aimed at CI ≥ 2.5 L/min/m2 using fluids, inotropes and red blood cells during the first 8 postoperative hours. The primary outcome was a composite endpoint of 30-day all-cause mortality and severe postoperative complications during the hospital stay. A meta-analysis was also conducted including all randomized trials of postoperative GDHT published from 1966 to May 2017.
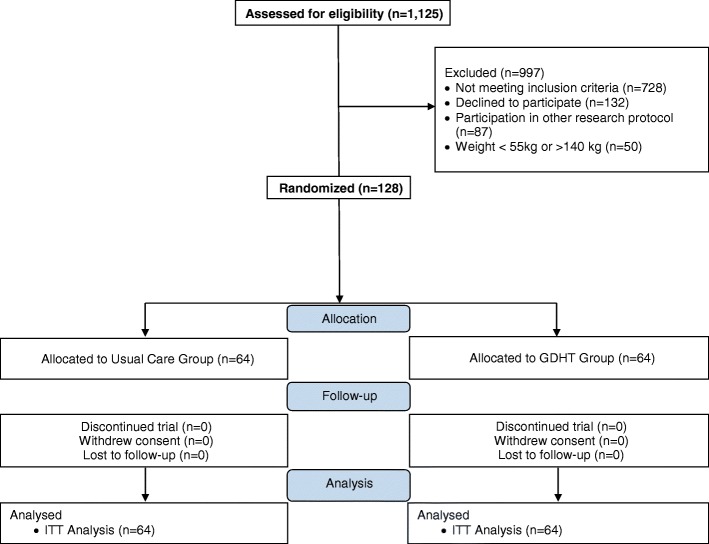
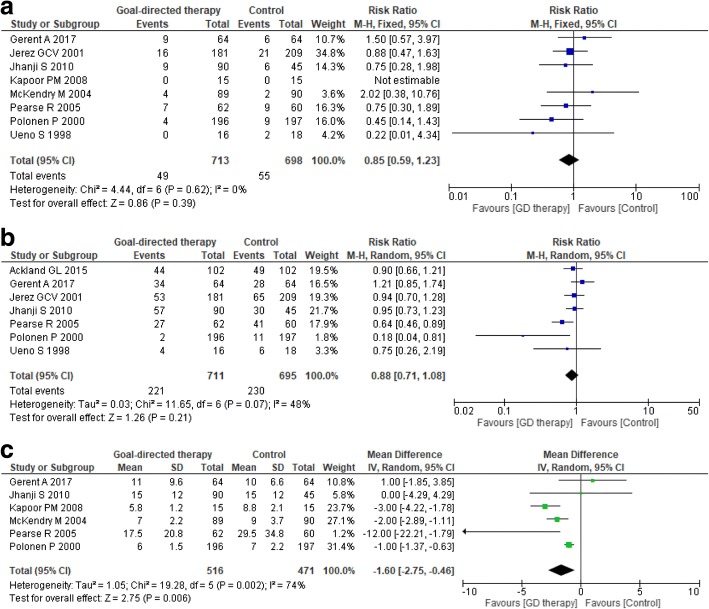
Results: A total of 128 patients (64 in each group) were randomized. The primary outcome occurred in 34 patients of the GDHT group and in 28 patients of the usual care group (53.1% vs 43.8%, absolute difference 9.4 (95% CI, - 7.8 to 25.8); p = 0.3). During the 8-h intervention period more patients in the GDHT group received dobutamine when compared to the usual care group (55% vs 16%, p < 0.001). A meta-analysis of nine randomized trials showed no differences in postoperative mortality (risk ratio 0.85, 95% CI 0.59-1.23; p = 0.4; p for heterogeneity = 0.7; I2 = 0%) and in the overall complications rate (risk ratio 0.88, 95% CI 0.71-1.08; p = 0.2; p for heterogeneity = 0.07; I2 = 48%), but a reduced hospital length of stay in the GDHT group (mean difference (MD) - 1.6; 95% CI - 2.75 to - 0.46; p = 0.006; p for heterogeneity = 0.002; I2 = 74%).
Conclusions: CI-guided hemodynamic therapy in the first 8 postoperative hours does not reduce 30-day mortality and severe complications during hospital stay when compared to usual care in cancer patients undergoing high-risk surgery.
Trial registration: www.clinicaltrials.gov , NCT01946269 . Registered on 16 September 2013.
Keywords: Cancer; Goal-directed therapy; High-risk surgery; Meta-analysis; Mortality; Randomized clinical trial.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Faculty of Medicine Ethics Committee (number 335/13). Written informed consent was obtained from all subjects or their legal surrogates prior to enrolment in the study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
