

A Simple, Evidence-Based Approach to Help Guide Diagnosis of Heart Failure With Preserved Ejection Fraction
- PMID: 29792299
- PMCID: PMC6202181
- DOI: 10.1161/CIRCULATIONAHA.118.034646
A Simple, Evidence-Based Approach to Help Guide Diagnosis of Heart Failure With Preserved Ejection Fraction
Abstract
Background: Diagnosis of heart failure with preserved ejection fraction (HFpEF) is challenging in euvolemic patients with dyspnea, and no evidence-based criteria are available. We sought to develop and then validate noninvasive diagnostic criteria that could be used to estimate the likelihood that HFpEF is present among patients with unexplained dyspnea to guide further testing.
Methods: Consecutive patients with unexplained dyspnea referred for invasive hemodynamic exercise testing were retrospectively evaluated. Diagnosis of HFpEF (case) or noncardiac dyspnea (control) was ascertained by invasive hemodynamic exercise testing. Logistic regression was performed to evaluate the ability of clinical findings to discriminate cases from controls. A scoring system was developed and then validated in a separate test cohort.
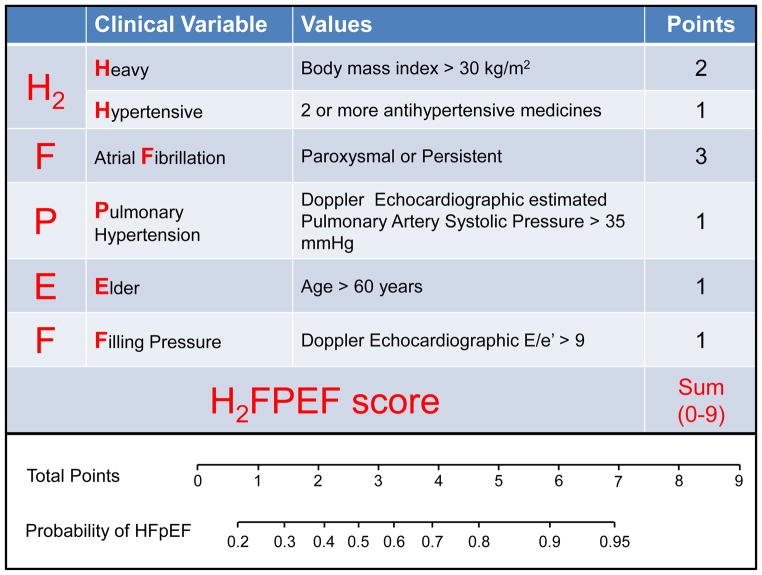
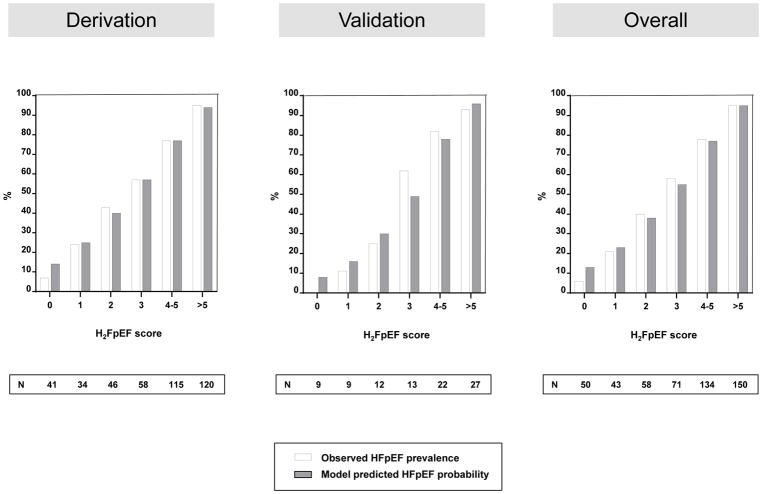
Results: The derivation cohort included 414 consecutive patients (267 cases with HFpEF and 147 controls; HFpEF prevalence, 64%). The test cohort included 100 consecutive patients (61 with HFpEF; prevalence, 61%). Obesity, atrial fibrillation, age >60 years, treatment with ≥2 antihypertensives, echocardiographic E/e' ratio >9, and echocardiographic pulmonary artery systolic pressure >35 mm Hg were selected as the final set of predictive variables. A weighted score based on these 6 variables was used to create a composite score (H2FPEF score) ranging from 0 to 9. The odds of HFpEF doubled for each 1-unit score increase (odds ratio, 1.98; 95% CI, 1.74-2.30; P<0.0001), with an area under the curve of 0.841 ( P<0.0001). The H2FPEF score was superior to a currently used algorithm based on expert consensus (increase in area under the curve of 0.169; 95% CI, 0.120-0.217; P<0.0001). Performance in the independent test cohort was maintained (area under the curve, 0.886; P<0.0001).
Conclusions: The H2FPEF score, which relies on simple clinical characteristics and echocardiography, enables discrimination of HFpEF from noncardiac causes of dyspnea and can assist in determination of the need for further diagnostic testing in the evaluation of patients with unexplained exertional dyspnea.
Keywords: catheterization; exercise test; heart failure.
Figures
Comment in
-
H2FPEF Score: At Last, a Properly Validated Diagnostic Algorithm for Heart Failure With Preserved Ejection Fraction.Circulation. 2018 Aug 28;138(9):871-873. doi: 10.1161/CIRCULATIONAHA.118.035711. Circulation. 2018. PMID: 30354456 No abstract available.
-
Response by Reddy and Borlaug to Letters Regarding Article, "A Simple, Evidence-Based Approach to Help Guide Diagnosis of Heart Failure With Preserved Ejection Fraction".Circulation. 2019 Feb 12;139(7):992-993. doi: 10.1161/CIRCULATIONAHA.118.038818. Circulation. 2019. PMID: 30742532 Free PMC article. No abstract available.
-
Letter by Cobos Gil Regarding Article, "A Simple, Evidence-Based Approach to Help Guide Diagnosis of Heart Failure With Preserved Ejection Fraction".Circulation. 2019 Feb 12;139(7):989. doi: 10.1161/CIRCULATIONAHA.118.037840. Circulation. 2019. PMID: 30742535 No abstract available.
-
Letter by Del Buono et al Regarding Article, "A Simple, Evidence-Based Approach To Help Guide Diagnosis of Heart Failure With Preserved Ejection Fraction".Circulation. 2019 Feb 12;139(7):990-991. doi: 10.1161/CIRCULATIONAHA.118.038072. Circulation. 2019. PMID: 30742537 No abstract available.
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Redfield MM. Heart failure with preserved ejection fraction. N Engl J Med. 2016;375:1868–1877. - PubMed
-
- Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, Marino P, Smiseth OA, De Keulenaer G, Leite-Moreira AF, Borbely A, Edes I, Handoko ML, Heymans S, Pezzali N, Pieske B, Dickstein K, Fraser AG, Brutsaert DL. How to diagnose diastolic heart failure: A consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the heart failure and echocardiography associations of the european society of cardiology. Eur Heart J. 2007;28:2539–2550. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 esc guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the european society of cardiology (esc) developed with the special contribution of the heart failure association (hfa) of the esc. Eur Heart J. 2016;37:2129–2200. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
