

Metabolic and Physiologic Imaging Biomarkers of the Tumor Microenvironment Predict Treatment Outcome with Radiation or a Hypoxia-Activated Prodrug in Mice
- PMID: 29792309
- PMCID: PMC8092078
- DOI: 10.1158/0008-5472.CAN-18-0491
Metabolic and Physiologic Imaging Biomarkers of the Tumor Microenvironment Predict Treatment Outcome with Radiation or a Hypoxia-Activated Prodrug in Mice
Abstract
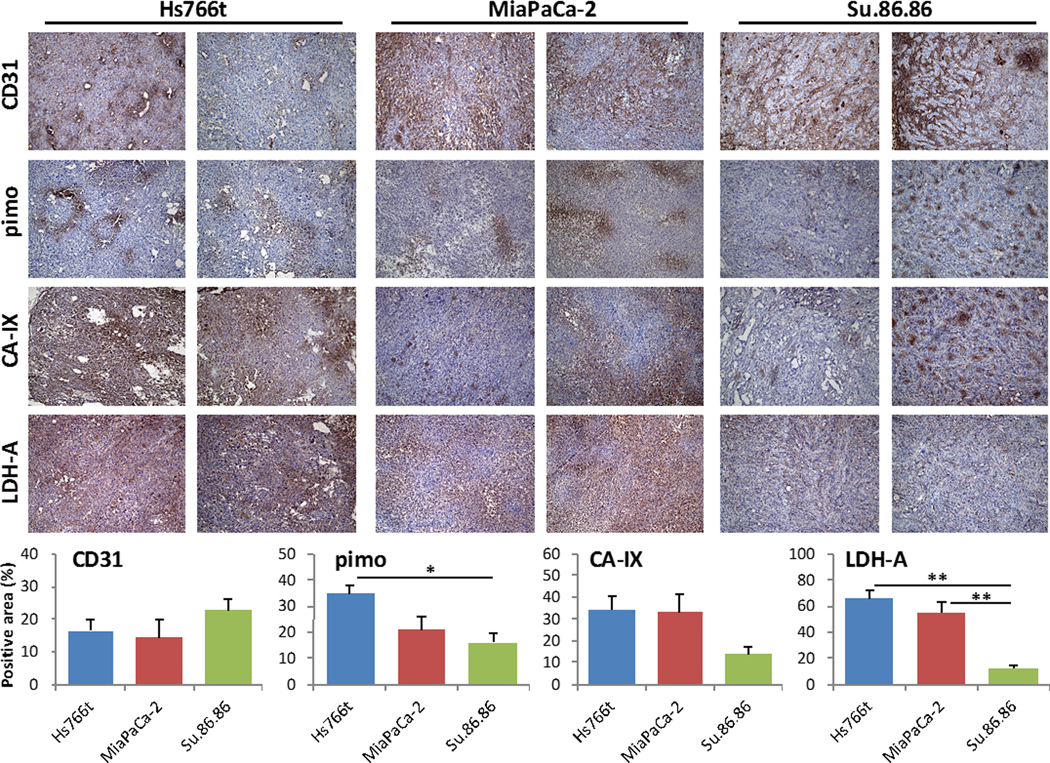
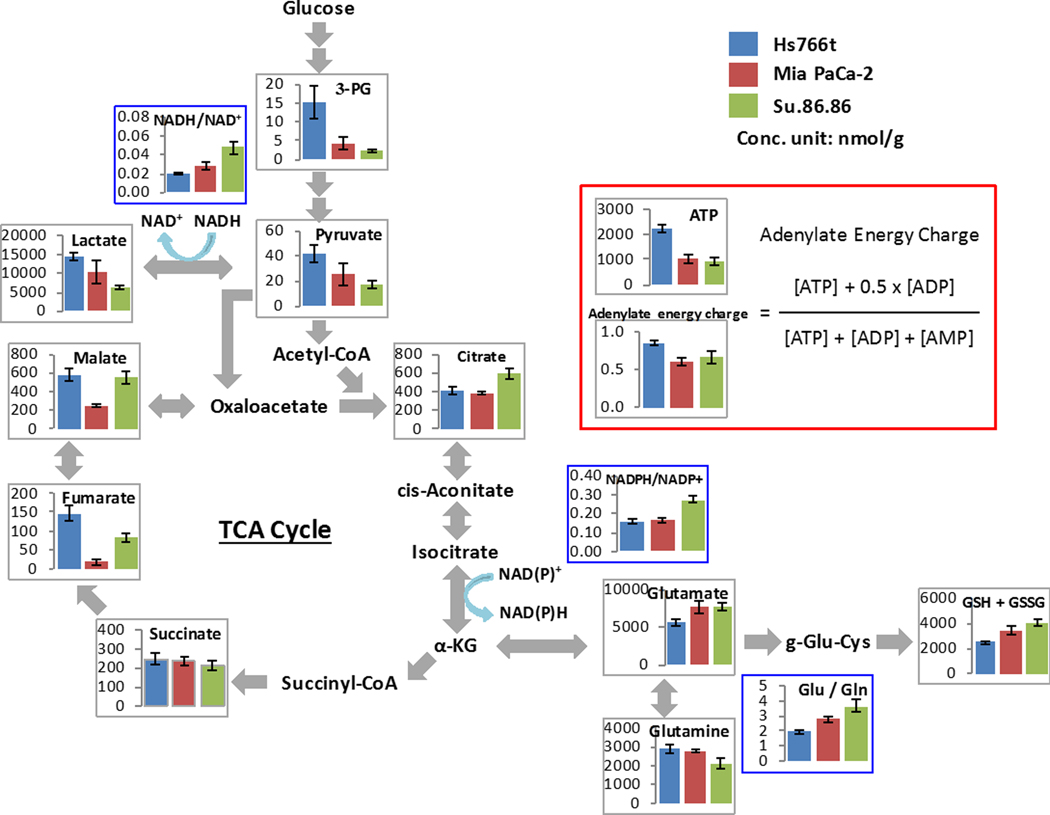
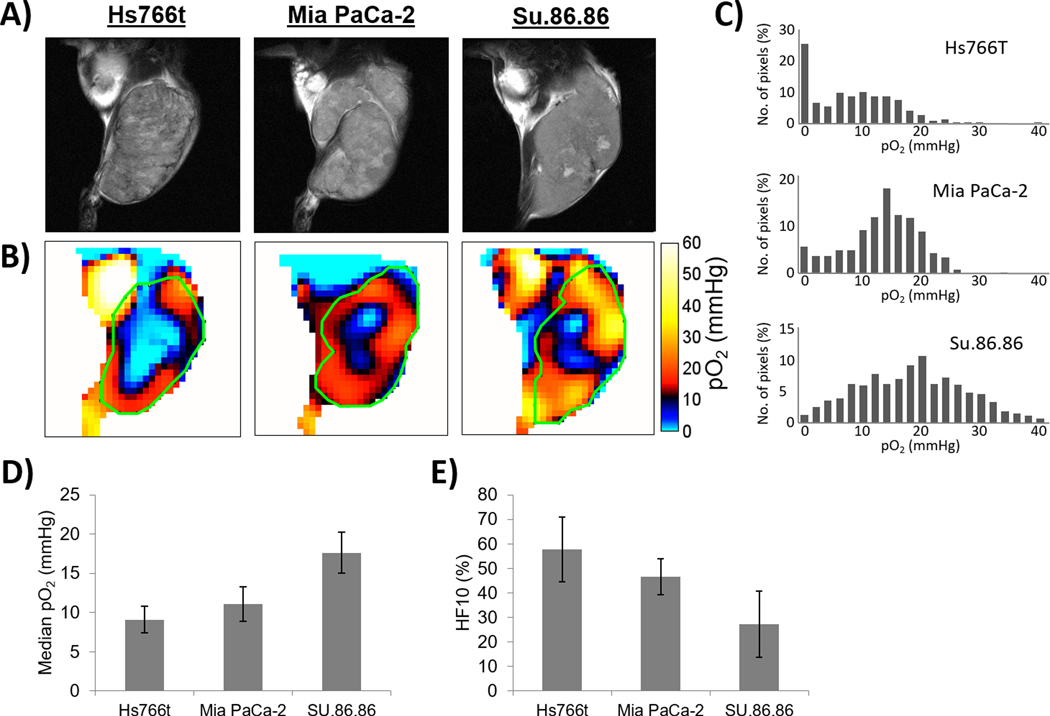
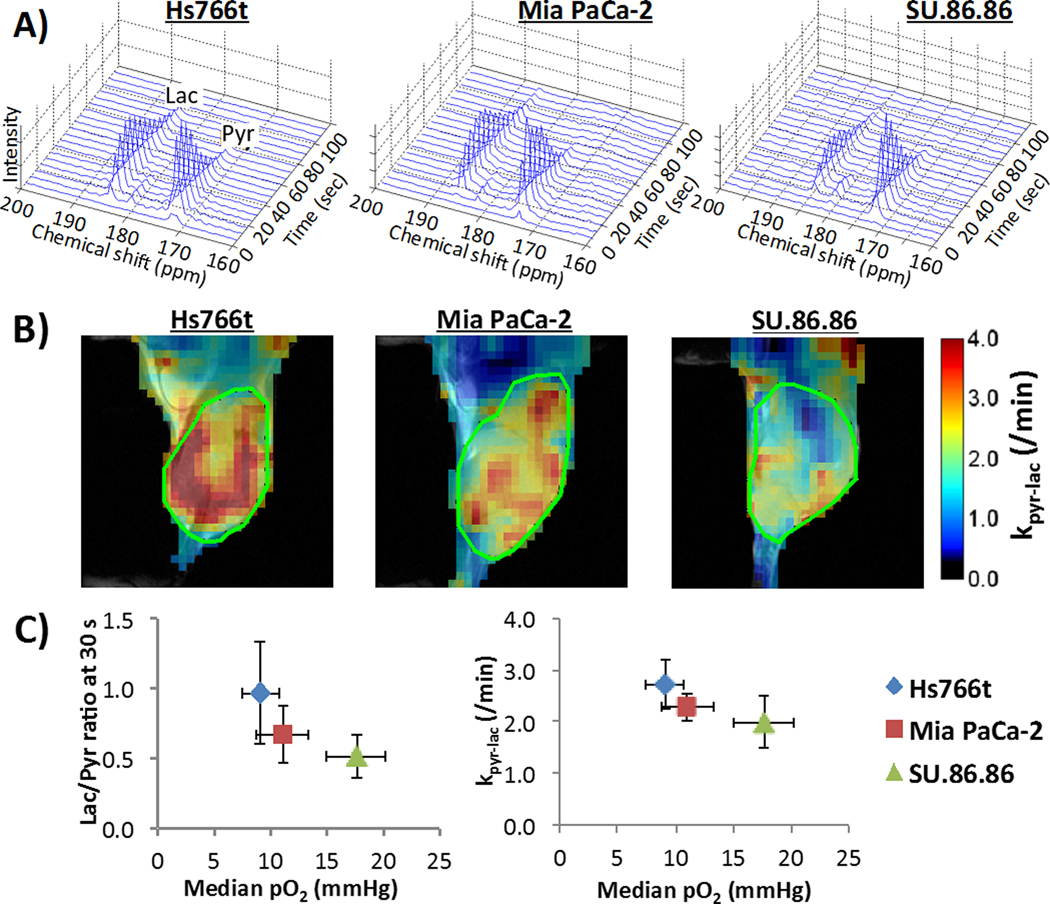
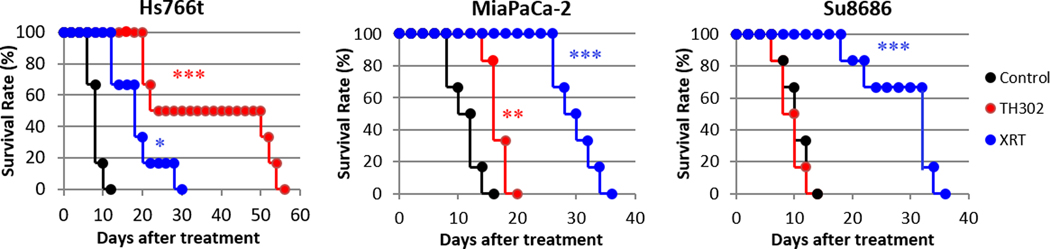
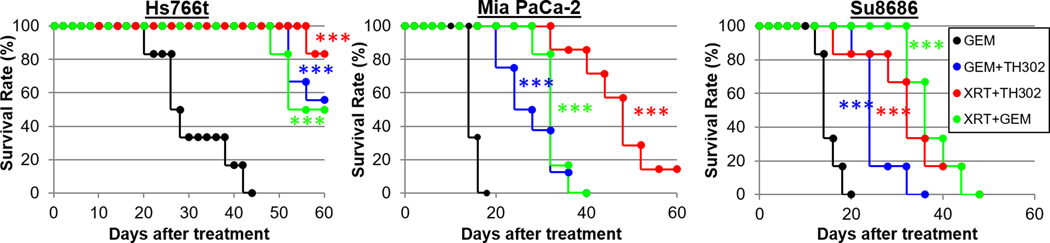
Pancreatic ductal adenocarcinoma (PDAC) is characterized by hypoxic niches that lead to treatment resistance. Therefore, studies of tumor oxygenation and metabolic profiling should contribute to improved treatment strategies. Here, we define two imaging biomarkers that predict differences in tumor response to therapy: (i) partial oxygen pressure (pO2), measured by EPR imaging; and (ii) [1-13C] pyruvate metabolism rate, measured by hyperpolarized 13C MRI. Three human PDAC xenografts with varying treatment sensitivity (Hs766t, MiaPaCa2, and Su.86.86) were grown in mice. The median pO2 of the mature Hs766t, MiaPaCa2, and Su.86.86 tumors was 9.1 ± 1.7, 11.1 ± 2.2, and 17.6 ± 2.6 mm Hg, and the rate of pyruvate-to-lactate conversion was 2.72 ± 0.48, 2.28 ± 0.26, and 1.98 ± 0.51 per minute, respectively (n = 6, each). These results are in agreement with steady-state data of matabolites quantified by mass spectroscopy and histologic analysis, indicating glycolytic and hypoxia profile in Hs766t, MiaPaca2, and Su.86.86 tumors. Fractionated radiotherapy (5 Gy × 5) resulted in a tumor growth delay of 16.7 ± 1.6 and 18.0 ± 2.7 days in MiaPaca2 and Su.86.86 tumors, respectively, compared with 6.3 ± 2.7 days in hypoxic Hs766t tumors. Treatment with gemcitabine, a first-line chemotherapeutic agent, or the hypoxia-activated prodrug TH-302 was more effective against Hs766t tumors (20.0 ± 3.5 and 25.0 ± 7.7 days increase in survival time, respectively) than MiaPaCa2 (2.7 ± 0.4 and 6.7 ± 0.7 days) and Su.86.86 (4.7 ± 0.6 and 0.7 ± 0.6 days) tumors. Collectively, these results demonstrate the ability of molecular imaging biomarkers to predict the response of PDAC to treatment with radiotherapy and TH-302.Significance: pO2 imaging data and clinically available metabolic imaging data provide useful insight into predicting the treatment efficacy of chemotherapy, radiation, and a hypoxia-activated prodrug as monotherapies and combination therapies in PDAC tumor xenograft models. Cancer Res; 78(14); 3783-92. ©2018 AACR.
©2018 American Association for Cancer Research.
Conflict of interest statement
The authors have declared that no conflict of interest exists.
Figures
References
-
- Hidalgo M, Von Hoff DD. Translational Therapeutic Opportunities in Ductal Adenocarcinoma of the Pancreas. Clin Cancer Res. 2012;18:4249–56. - PubMed
-
- Stathis A, Moore MJ. Advanced pancreatic carcinoma: current treatment and future challenges. Nat Rev Clin Oncol; 2010;7:163–72. - PubMed
-
- Erkan M, Hausmann S, Michalski CW, Fingerle AA, Dobritz M, Kleeff J, et al. The role of stroma in pancreatic cancer: diagnostic and therapeutic implications. Nat Rev Gastroenterol Hepatol; 2012;9:454–67. - PubMed
-
- Koong AC, Mehta VK, Le QT, Fisher GA, Terris DJ, Brown JM, et al. Pancreatic tumors show high levels of hypoxia. Int J Radiat Oncol Biol Phys. 2000;48:919–22. - PubMed
-
- Matsuo Y, Ding Q, Desaki R, Maemura K, Mataki Y, Shinchi H, et al. Hypoxia inducible factor-1 alpha plays a pivotal role in hepatic metastasis of pancreatic cancer: an immunohistochemical study. J Hepatobiliary Pancreat Sci. 2014;21:105–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
