

An assessment of public health surveillance of Zika virus infection and potentially associated outcomes in Latin America
- PMID: 29793453
- PMCID: PMC5968501
- DOI: 10.1186/s12889-018-5566-7
An assessment of public health surveillance of Zika virus infection and potentially associated outcomes in Latin America
Abstract
Background: We evaluated whether outbreaks of Zika virus (ZIKV) infection, newborn microcephaly, and Guillain-Barré syndrome (GBS) in Latin America may be detected through current surveillance systems, and how cases detected through surveillance may increase health care burden.
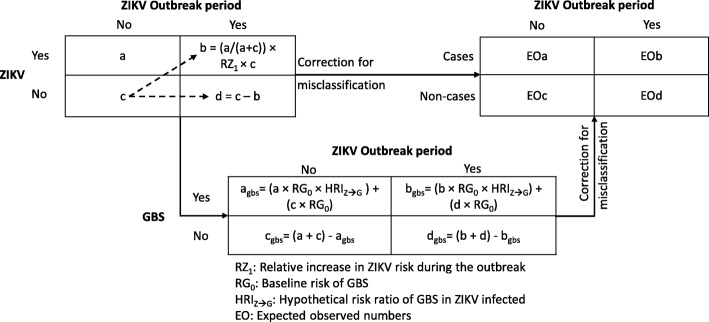
Methods: We estimated the sensitivity and specificity of surveillance case definitions using published data. We assumed a 10% ZIKV infection risk during a non-outbreak period and hypothetical increases in risk during an outbreak period. We used sensitivity and specificity estimates to correct for non-differential misclassification, and calculated a misclassification-corrected relative risk comparing both periods. To identify the smallest hypothetical increase in risk resulting in a detectable outbreak we compared the misclassification-corrected relative risk to the relative risk corresponding to the upper limit of the endemic channel (mean + 2 SD). We also estimated the proportion of false positive cases detected during the outbreak. We followed the same approach for microcephaly and GBS, but assumed the risk of ZIKV infection doubled during the outbreak, and ZIKV infection increased the risk of both diseases.
Results: ZIKV infection outbreaks were not detectable through non-serological surveillance. Outbreaks were detectable through serologic surveillance if infection risk increased by at least 10%, but more than 50% of all cases were false positive. Outbreaks of severe microcephaly were detected if ZIKV infection increased prevalence of this condition by at least 24.0 times. When ZIKV infection did not increase the prevalence of severe microcephaly, 34.7 to 82.5% of all cases were false positive, depending on diagnostic accuracy. GBS outbreaks were detected if ZIKV infection increased the GBS risk by at least seven times. For optimal GBS diagnosis accuracy, the proportion of false positive cases ranged from 29 to 54% and from 45 to 56% depending on the incidence of GBS mimics.
Conclusions: Current surveillance systems have a low probability of detecting outbreaks of ZIKV infection, severe microcephaly, and GBS, and could result in significant increases in health care burden, due to the detection of large numbers of false positive cases. In view of these limitations, Latin American countries should consider alternative options for surveillance.
Conflict of interest statement
Authors’ information
LB is a physician epidemiologist, with a DrPH in Epidemiology from Johns Hopkins University (infectious diseases). He is currently an Associate Professor at the University of Wisconsin, Madison, and his main research resides on the impact of cardiovascular diseases in Latin America. VMH is a physician epidemiologist, with a PhD in Epidemiology from the University of Wisconsin, currently Associate Professor at the Universidad Autónoma de Bucaramanga, Colombia. His research is mostly focused on dengue and Zika virus infections.
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Pan American Health O . Guidelines for Zika virus disease and complications surveillance. Washington, D.C.: PAHO; 2016.
-
- World Health O. Surveillance for Zika virus infection, microcephaly and Guillain-Barré syndrome: interim guidance. 2016.
-
- Cuevas EL, Tong VT, Rozo N, Valencia D, Pacheco O, Gilboa SM, Mercado M, Renquist CM, González M, Ailes EC. Preliminary report of microcephaly potentially associated with Zika virus infection during pregnancy-Colombia, January-November 2016. MMWRMorbidity and mortality weekly report. 2016;65(49):1409. doi: 10.15585/mmwr.mm6549e1. - DOI - PubMed
-
- Bautista LE: On the temporal association of outbreaks of Zika virus infection, newborn microcephaly, and Guillain-Barré syndrome. J Public Health Emerg; July 2017 2017.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
