

Antidepressant utilisation and incidence of weight gain during 10 years' follow-up: population based cohort study
- PMID: 29793997
- PMCID: PMC5964332
- DOI: 10.1136/bmj.k1951
Antidepressant utilisation and incidence of weight gain during 10 years' follow-up: population based cohort study
Abstract
Objective: To evaluate the long term association between antidepressant prescribing and body weight.
Design: Population based cohort study.
Setting: General practices contributing to the UK Clinical Practice Research Datalink, 2004-14.
Participants: 136 762 men and 157 957 women with three or more records for body mass index (BMI).
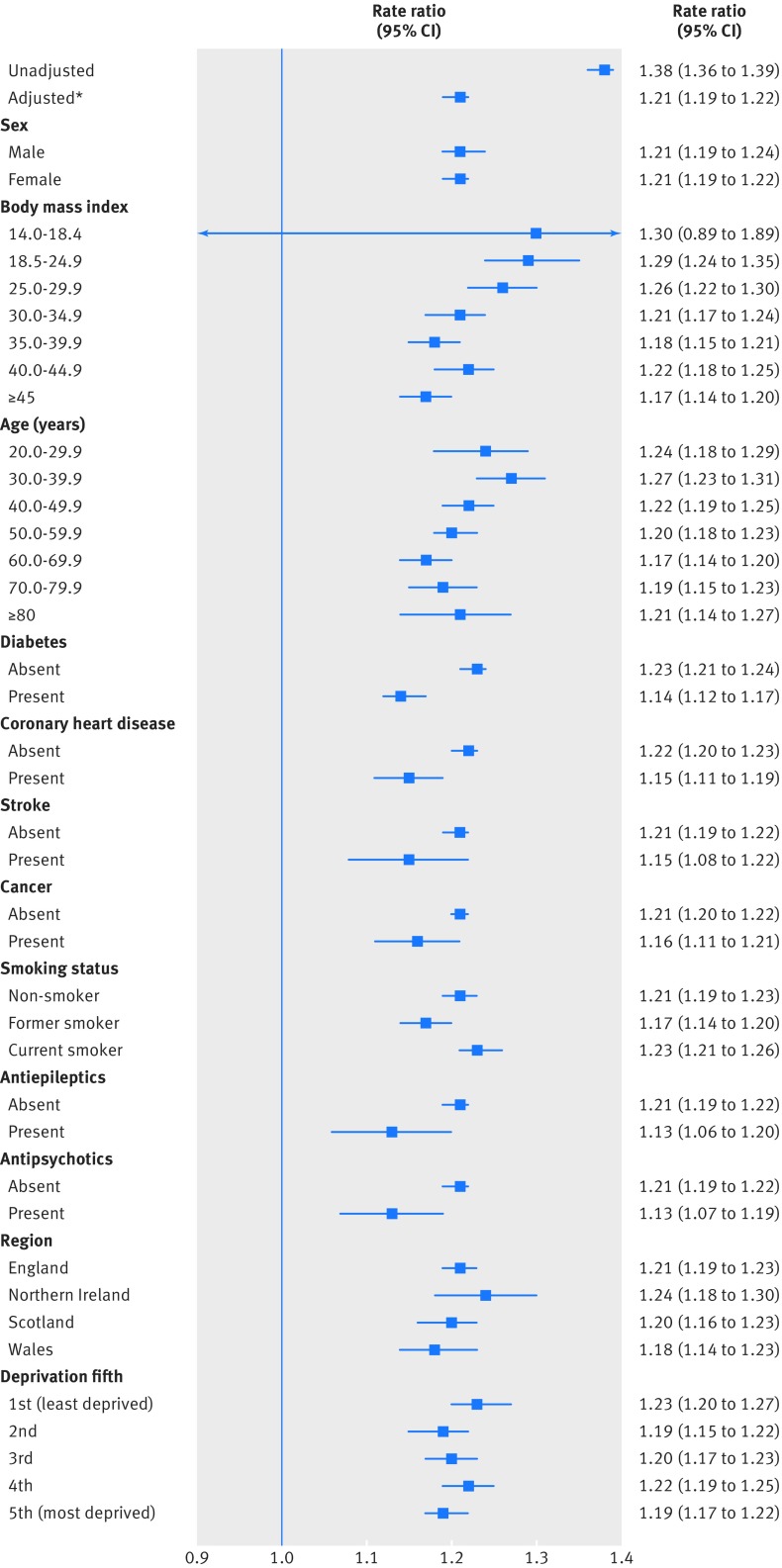
Main outcome measures: The main outcomes were antidepressant prescribing, incidence of ≥5% increase in body weight, and transition to overweight or obesity. Adjusted rate ratios were estimated from a Poisson model adjusting for age, sex, depression recording, comorbidity, coprescribing of antiepileptics or antipsychotics, deprivation, smoking, and advice on diet.
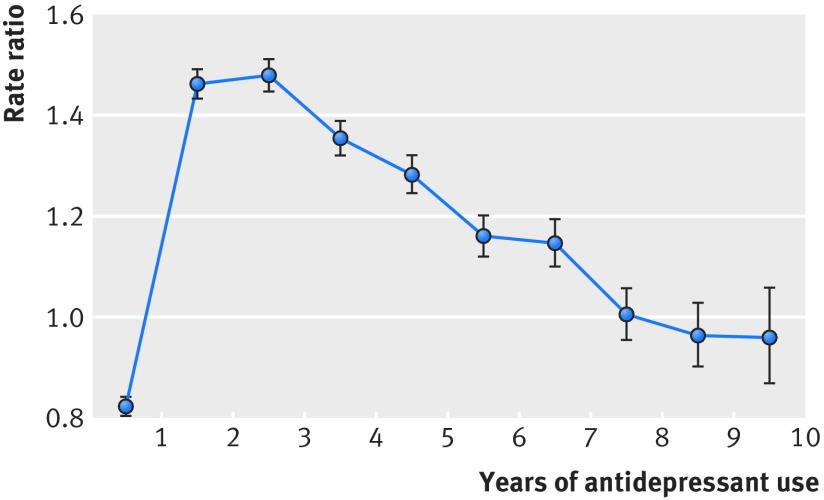
Results: In the year of study entry, 17 803 (13.0%) men and 35 307 (22.4%) women with a mean age of 51.5 years (SD 16.6 years) were prescribed antidepressants. During 1 836 452 person years of follow-up, the incidence of new episodes of ≥5 weight gain in participants not prescribed antidepressants was 8.1 per 100 person years and in participants prescribed antidepressants was 11.2 per 100 person years (adjusted rate ratio 1.21, 95% confidence interval 1.19 to 1.22, P<0.001). The risk of weight gain remained increased during at least six years of follow-up. In the second year of treatment the number of participants treated with antidepressants for one year for one additional episode of ≥5% weight gain was 27 (95% confidence interval 25 to 29). In people who were initially of normal weight, the adjusted rate ratio for transition to overweight or obesity was 1.29 (1.25 to 1.34); in people who were initially overweight, the adjusted rate ratio for transition to obesity was 1.29 (1.25 to 1.33). Associations may not be causal, and residual confounding might contribute to overestimation of associations.
Conclusion: Widespread utilisation of antidepressants may be contributing to long term increased risk of weight gain at population level. The potential for weight gain should be considered when antidepressant treatment is indicated.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf. HPB is now employed by CPRD; there are no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; and no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- Joint Health Surveys Unit Health Survey for England: trend tables 2016. NHS Information Centre, 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical