

An Observational Cohort Study of Clostridium difficile Ribotype 027 and Recurrent Infection
- PMID: 29794054
- PMCID: PMC5967198
- DOI: 10.1128/mSphere.00033-18
An Observational Cohort Study of Clostridium difficile Ribotype 027 and Recurrent Infection
Abstract
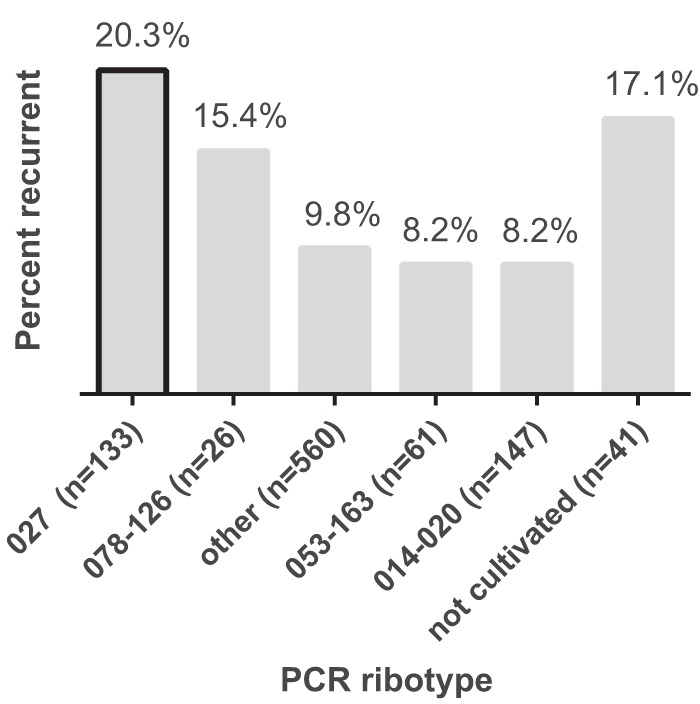
Recurrent Clostridium difficile infection (rCDI) frequently complicates recovery from CDI. Accurately predicting rCDI would allow judicious allocation of limited resources, but published models have met with limited success. Thus, biomarkers predictive of recurrence have been sought. This study tested whether PCR ribotype independently predicted rCDI. Stool samples from nonpregnant inpatients ≥18 years of age with diarrhea were included from October 2010 to January 2013 after the patients tested positive for C. difficile in the clinical microbiology laboratory. Per guidelines, the rCDI was defined as a positive test for C. difficile at >2 weeks but ≤8 weeks from the index episode. For each sample, a single colony of C. difficile was isolated by anaerobic culture, confirmed to be toxigenic by PCR, and ribotyped. Simple logistic regression and multiple logistic regression were used to model the primary outcome of rCDI, incorporating a wide range of clinical parameters. In total, 927 patients with 968 index episodes of CDI were included, with 110 (11.4%) developing rCDI. Age and use of proton pump inhibitors or concurrent antibiotics did not increase the risk of rCDI. Low serum bilirubin levels and ribotype 027 were associated with increased risk of rCDI on unadjusted analysis, with health care-associated CDI being inversely associated. In the final multivariable model, ribotype 027 was the strongest independent predictor of rCDI (odds ratio, 2.17; 95% confidence interval, 1.33 to 3.56; P = 0.002). Ribotype 027 is an independent predictor of rCDI.IMPORTANCE CDI is a major public health issue, with over 400,000 cases per year in the United States alone. Recurrent CDI is common, occurring in approximately one in five individuals after a primary episode. Although interventions exist that could reduce the risk of recurrence, deployment in all patients is limited by cost, invasiveness, and/or an undetermined long-term safety profile. Thus, clinicians need risk stratification tools to properly allocate treatments. Because prior research on clinical predictors has failed to yield a reliable, reproducible, and effective predictive model to assist treatment decisions, accurate biomarkers of recurrence would be of great value. This study tested whether PCR ribotype independently predicted rCDI, and the data build upon prior research in showing that ribotype 027 is associated with rCDI.
Keywords: Clostridium difficile; biomarkers; clinical decision making; molecular epidemiology; ribotyping.
Copyright © 2018 Rao et al.
Figures
Similar articles
-
Molecular epidemiology of toxigenic Clostridioides difficile isolates from hospitalized patients and the hospital environment in Dhaka, Bangladesh.Anaerobe. 2020 Feb;61:102081. doi: 10.1016/j.anaerobe.2019.102081. Epub 2019 Jul 26. Anaerobe. 2020. PMID: 31356958 Free PMC article.
-
Epidemiology of Clostridioides difficile PCR ribotype 181 after the COVID-19 pandemic in Northern Greece.Acta Microbiol Immunol Hung. 2024 Oct 28;71(4):315-323. doi: 10.1556/030.2024.02401. Print 2024 Dec 19. Acta Microbiol Immunol Hung. 2024. PMID: 39466344
-
Clostridium difficile infection in patients with inflammatory bowel disease: a case control study.Scand J Gastroenterol. 2018 Aug;53(8):947-951. doi: 10.1080/00365521.2018.1492012. Epub 2018 Jul 25. Scand J Gastroenterol. 2018. PMID: 30041549
-
Burden of Clostridioides difficile infection (CDI) - a systematic review of the epidemiology of primary and recurrent CDI.BMC Infect Dis. 2021 May 19;21(1):456. doi: 10.1186/s12879-021-06147-y. BMC Infect Dis. 2021. PMID: 34016040 Free PMC article.
-
The burden of Clostridioides difficile infections in South-East Asia and the Western Pacific: A narrative review.Anaerobe. 2024 Apr;86:102821. doi: 10.1016/j.anaerobe.2024.102821. Epub 2024 Feb 7. Anaerobe. 2024. PMID: 38336258 Review.
Cited by
-
Chronic Rifaximin Use in Cirrhotic Patients Is Associated with Decreased Rate of C. difficile Infection.Dig Dis Sci. 2020 Feb;65(2):632-638. doi: 10.1007/s10620-019-05804-2. Epub 2019 Aug 22. Dig Dis Sci. 2020. PMID: 31440997
-
Prevalence of diagnostically-discrepant Clostridioides difficile clinical specimens: insights from longitudinal surveillance.Front Med (Lausanne). 2023 Oct 18;10:1238159. doi: 10.3389/fmed.2023.1238159. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37928470 Free PMC article.
-
Immune Profiling To Predict Outcome of Clostridioides difficile Infection.mBio. 2020 May 26;11(3):e00905-20. doi: 10.1128/mBio.00905-20. mBio. 2020. PMID: 32457246 Free PMC article.
-
An Update on Clostridioides difficile Binary Toxin.Toxins (Basel). 2022 Apr 27;14(5):305. doi: 10.3390/toxins14050305. Toxins (Basel). 2022. PMID: 35622552 Free PMC article. Review.
-
Transcriptomic analysis of biofilm formation in strains of Clostridioides difficile associated with recurrent and non-recurrent infection reveals potential candidate markers for recurrence.PLoS One. 2023 Aug 3;18(8):e0289593. doi: 10.1371/journal.pone.0289593. eCollection 2023. PLoS One. 2023. PMID: 37535660 Free PMC article.
References
-
- Lessa FC, Mu Y, Bamberg WM, Beldavs ZG, Dumyati GK, Dunn JR, Farley MM, Holzbauer SM, Meek JI, Phipps EC, Wilson LE, Winston LG, Cohen JA, Limbago BM, Fridkin SK, Gerding DN, McDonald LC. 2015. Burden of Clostridium difficile infection in the United States. N Engl J Med 372:825–834. doi:10.1056/NEJMoa1408913. - DOI - PMC - PubMed
-
- Crook DW, Walker AS, Kean Y, Weiss K, Cornely OA, Miller MA, Esposito R, Louie TJ, Stoesser NE, Young BC, Angus BJ, Gorbach SL, Peto TEA, Study 003/004 Teams . 2012. Fidaxomicin versus vancomycin for Clostridium difficile infection: meta-analysis of pivotal randomized controlled trials. Clin Infect Dis 55:S93–S103. doi:10.1093/cid/cis499. - DOI - PMC - PubMed
-
- Wilcox MH, Gerding DN, Poxton IR, Kelly C, Nathan R, Birch T, Cornely OA, Rahav G, Bouza E, Lee C, Jenkin G, Jensen W, Kim YS, Yoshida J, Gabryelski L, Pedley A, Eves K, Tipping R, Guris D, Kartsonis N, Dorr MB; MODIFY I and MODIFY II Investigators . 2017. Bezlotoxumab for prevention of recurrent Clostridium difficile infection. N Engl J Med 376:305–317. doi:10.1056/NEJMoa1602615. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
