

Frequency, risk factors, and impact on mortality of arterial thromboembolism in patients with cancer
- PMID: 29794142
- PMCID: PMC6119137
- DOI: 10.3324/haematol.2018.192419
Frequency, risk factors, and impact on mortality of arterial thromboembolism in patients with cancer
Abstract
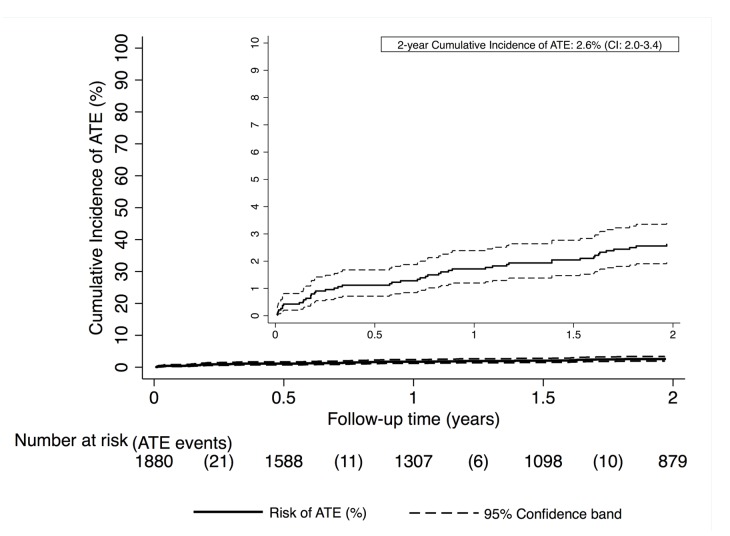
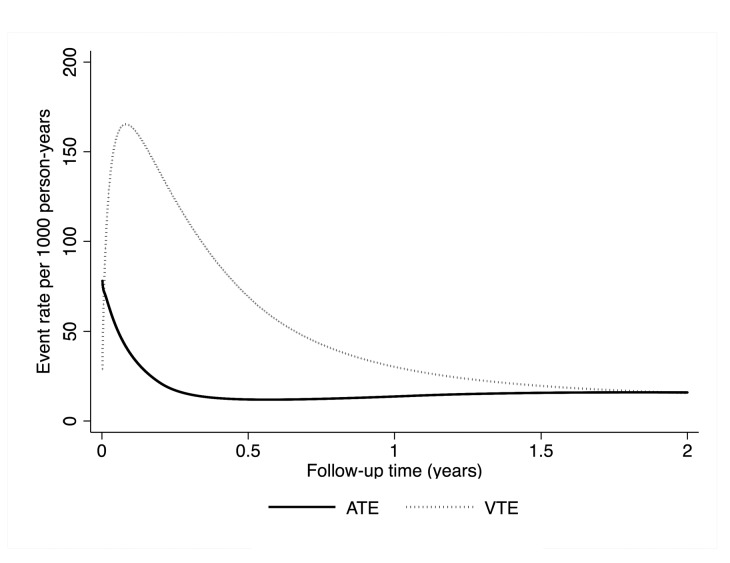
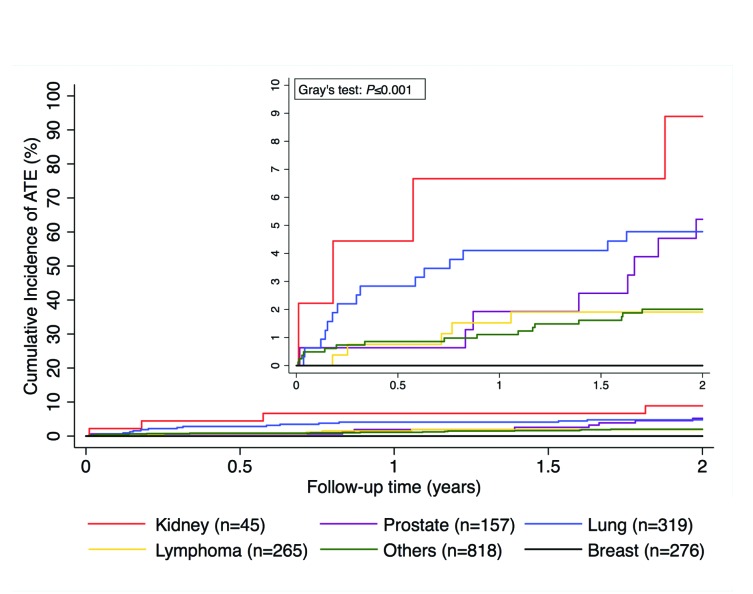
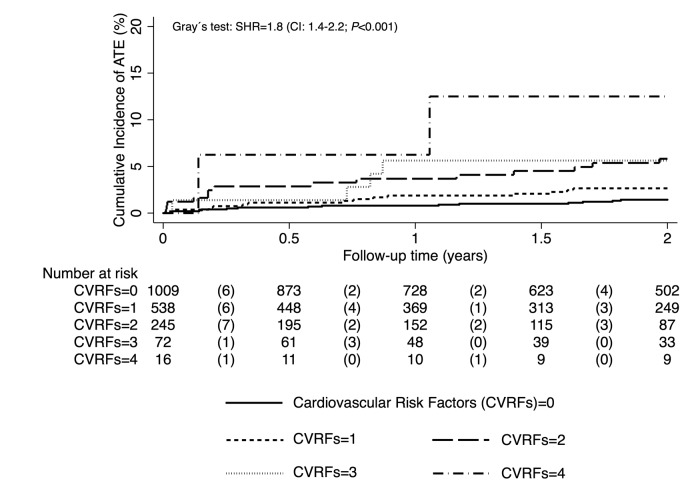
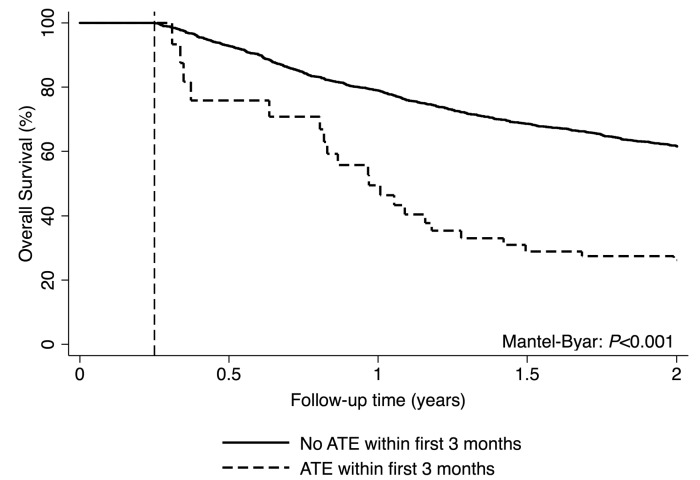
In contrast to venous thromboembolism, little is known about arterial thromboembolism in patients with cancer. The aim of this study was to quantify the risk and explore clinical risk factors of arterial thromboembolism in patients with cancer, and investigate its potential impact on mortality. Patients with newly-diagnosed cancer or progression of disease after remission were included in a prospective observational cohort study and followed for two years. Between October 2003 and October 2013, 1880 patients (54.3% male; median age 61 years) were included. During a median follow up of 723 days, 48 (2.6%) patients developed arterial thromboembolism [20 (41.7%) myocardial infarction, 16 (33.3%) stroke and 12 (25.0%) peripheral arterial events], 157 (8.4%) developed venous thromboembolism, and 754 (40.1%) patients died. The cumulative 3-, 6-, 12-, and 24-month risks of arterial thromboembolism were 0.9%, 1.1%, 1.7%, and 2.6%, respectively. Male sex (subdistribution hazard ratio=2.9, 95%CI: 1.5-5.6; P=0.002), age (subdistribution hazard ratio per 10 year increase=1.5, 1.2-1.7; P<0.001), hypertension (3.1, 1.7-5.5; P<0.001), smoking (2.0, 1.1-3.7; P=0.022), lung cancer (2.3, 1.2-4.2; P=0.009), and kidney cancer (3.8, 1.4-10.5; P=0.012) were associated with a higher arterial thromboembolism risk. Furthermore, the occurrence of arterial thromboembolism was associated with a 3.2-fold increased risk of all-cause mortality (hazard ratio=3.2, 95%CI: 2.2-4.8; P<0.001). Arterial thromboembolism is a less common complication in patients with cancer than venous thromboembolism. The risk of arterial thromboembolism is high in patients with lung and kidney cancer. Patients with cancer who develop arterial thromboembolism are at a 3-fold increased risk of mortality.
Copyright© 2018 Ferrata Storti Foundation.
Figures
Comment in
-
Arterial thrombosis and cancer: the neglected side of the coin of Trousseau syndrome.Haematologica. 2018 Sep;103(9):1419-1421. doi: 10.3324/haematol.2018.197814. Haematologica. 2018. PMID: 30171017 Free PMC article. No abstract available.
References
-
- Ay C, Pabinger I. Predictive potential of haemostatic biomarkers for venous thromboembolism in cancer patients. Thromb Res. 2012;129 Suppl 1:S6–9. - PubMed
-
- Riedl J, Pabinger I, Ay C. Platelets in cancer and thrombosis. Hamostaseologie. 2014;34(1):54–62. - PubMed
-
- Pabinger I, Thaler J, Ay C. Biomarkers for prediction of venous thromboembolism in cancer. Blood. 2013;122(12):2011–2018. - PubMed
-
- Königsbrügge O, Pabinger I, Ay C. Risk factors for venous thromboembolism in cancer: novel findings from the Vienna Cancer and Thrombosis Study (CATS). Thromb Res. 2014;133 Suppl 2:S39–43. - PubMed
-
- Di Nisio M, Ferrante N, Feragalli B, et al. Arterial thrombosis in ambulatory cancer patients treated with chemotherapy. Thromb Res. 2011;127(4):382–383. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
