

Multiple intracranial lesions as the unusual imaging features of Hashimoto's encephalopathy: A case report
- PMID: 29794766
- PMCID: PMC6393037
- DOI: 10.1097/MD.0000000000010814
Multiple intracranial lesions as the unusual imaging features of Hashimoto's encephalopathy: A case report
Abstract
Rationale: Hashimoto's encephalopathy (HE) is associated with autoimmune thyroid disease and is complex, diverse, and easily misdiagnosed. However, if HE is diagnosed and treated in a timely manner, an optimal prognosis may be achieved.
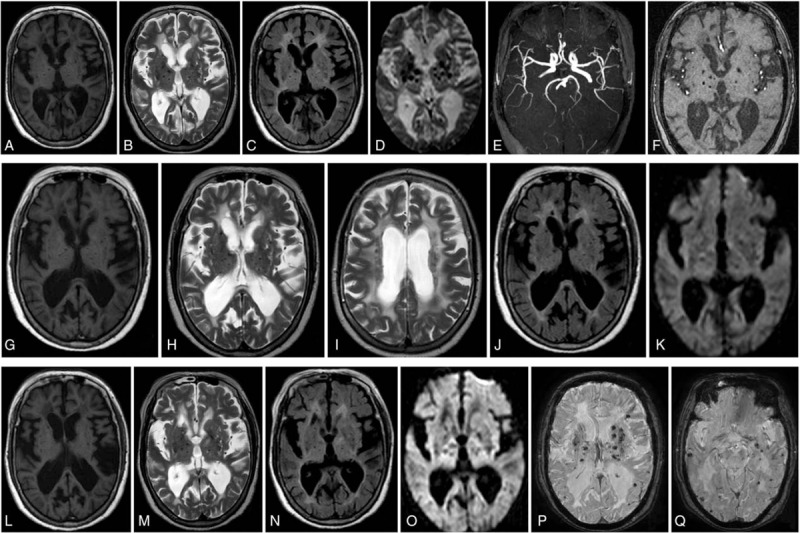
Patient concerns: We presented a case of a 63-year-old female patient with paroxysmal dizziness, unsteady gait, emotion apathy, progressive cognitive impairment, and unusual magnetic resonance imaging (MRI) findings.
Diagnoses: After suffering for almost 8 years, the patient was diagnosed with HE based on clinical manifestation, abnormal electroencephalogram, unusual MRI findings, sensitivity to cortisol treatment, and characteristic high antithyroid peroxidase antibody (TpoAb) titer.
Interventions: The patient continued regular glucocorticoids therapy after intravenous methylprednisolone pulse therapy, neurotrophic drugs, traditional Chinese medicine and rehabilitation to relieve hypermyotonia and cognitive impairment.
Outcomes: After combined treatment, the patient's symptoms, electroencephalogram (EEG), MRI, and the TpoAb titer gradually improved. However, the patient had to stop glucocorticoids treatment because of severe osteoporosis, fractures and other adverse reactions. Her symptoms fluctuated, and her TpoAb titer increased again.
Lessons: HE may cause highly heterogeneous clinical features, particularly MRI findings. Withdrawal of the systematic glucocorticoids treatment can lead to varied outcomes in these patients.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


References
-
- Jia J, Chen S. Neurology. Beijing: People's Medical Publishing House; 2014.
-
- Peschen-Rosin R, Schabet M, Dichgans J. Manifestation of Hashimoto's encephalopathy years before onset of thyroid disease. Eur Neurol 1999;41:79–84. - PubMed
-
- Brain L, Jellinek EH, Ball K. Hashimoto's disease and encephalopathy. Lancet 1966;2:512–4. - PubMed
-
- Ferracci F, Bertiato G, Moretto G. Hashimoto's encephalopathy: epidemiologic data and pathogenetic considerations. J Neurol Sci 2004;217:165–8. - PubMed
-
- Passarella B, Negro C, Nozzoli C, et al. Cerebellar subacute syndrome due to corticosteroid-responsive encephalopathy associated with autoimmune thyroiditis (also called “Hashimoto's encephalopathy”). Clin Ter 2005;156:13–7. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
