

Myelodysplastic syndromes current treatment algorithm 2018
- PMID: 29795386
- PMCID: PMC5967332
- DOI: 10.1038/s41408-018-0085-4
Myelodysplastic syndromes current treatment algorithm 2018
Abstract
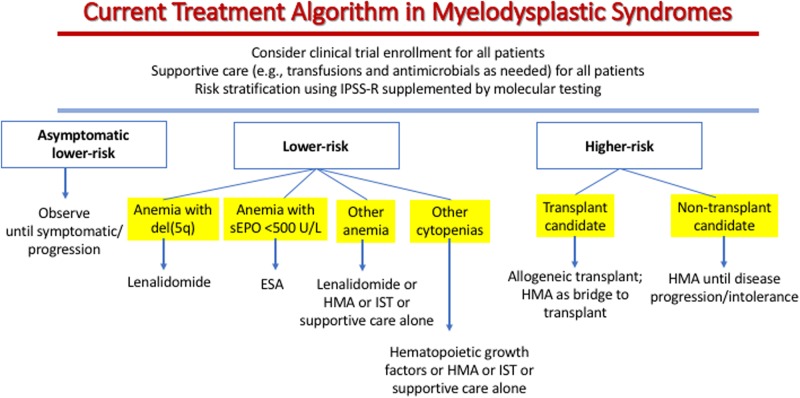
Myelodysplastic syndromes (MDS) include a group of clonal myeloid neoplasms characterized by cytopenias due to ineffective hematopoiesis, abnormal blood and marrow cell morphology, and a risk of clonal evolution and progression to acute myeloid leukemia (AML). Because outcomes for patients with MDS are heterogeneous, individual risk stratification using tools such as the revised International Prognostic Scoring System (IPSS-R) is important in managing patients-including selecting candidates for allogeneic hematopoietic stem cell transplantation (ASCT), the only potentially curative therapy for MDS. The IPSS-R can be supplemented by molecular genetic testing, since certain gene mutations such as TP53 influence risk independent of established clinicopathological variables. For lower risk patients with symptomatic anemia, treatment with erythropoiesis-stimulating agents (ESAs) or lenalidomide (especially for those with deletion of chromosome 5q) can ameliorate symptoms. Some lower risk patients may be candidates for immunosuppressive therapy, thrombopoiesis-stimulating agents, or a DNA hypomethylating agent (HMA; azacitidine or decitabine). Among higher risk patients, transplant candidates should undergo ASCT as soon as possible, with HMAs useful as a bridge to transplant. Non-transplant candidates should initiate HMA therapy and continue if tolerated until disease progression. Supportive care with transfusions and antimicrobial drugs as needed remains important in all groups.
Conflict of interest statement
Data safety monitoring committee: Janssen, Onconova, Takeda. Research support: H3 Biosciences, Celgene. Advisory board: Otsuka, Amphivena.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
