

Insights into the genetic epidemiology of Crohn's and rare diseases in the Ashkenazi Jewish population
- PMID: 29795570
- PMCID: PMC5967709
- DOI: 10.1371/journal.pgen.1007329
Insights into the genetic epidemiology of Crohn's and rare diseases in the Ashkenazi Jewish population
Erratum in
-
Correction: Insights into the genetic epidemiology of Crohn's and rare diseases in the Ashkenazi Jewish population.PLoS Genet. 2019 May 30;15(5):e1008190. doi: 10.1371/journal.pgen.1008190. eCollection 2019 May. PLoS Genet. 2019. PMID: 31145742 Free PMC article.
Abstract
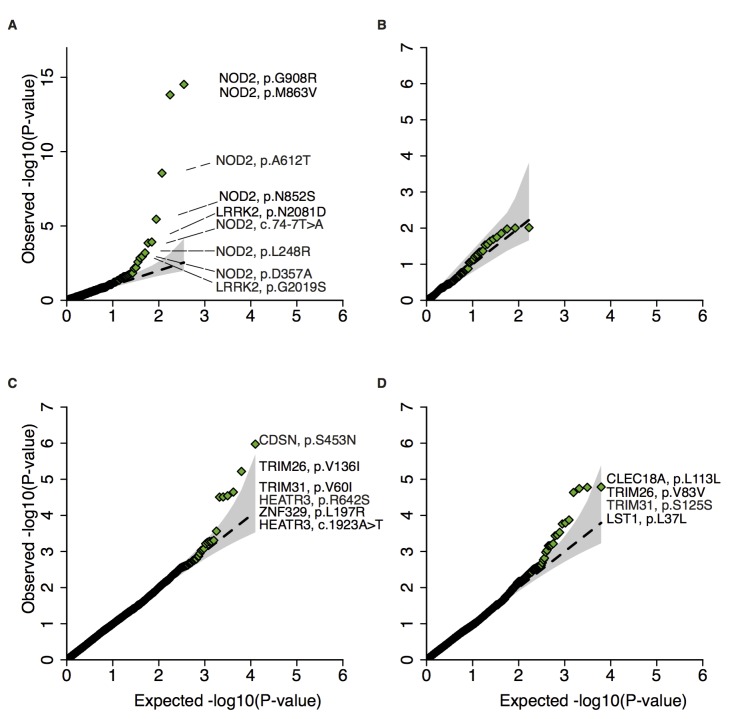
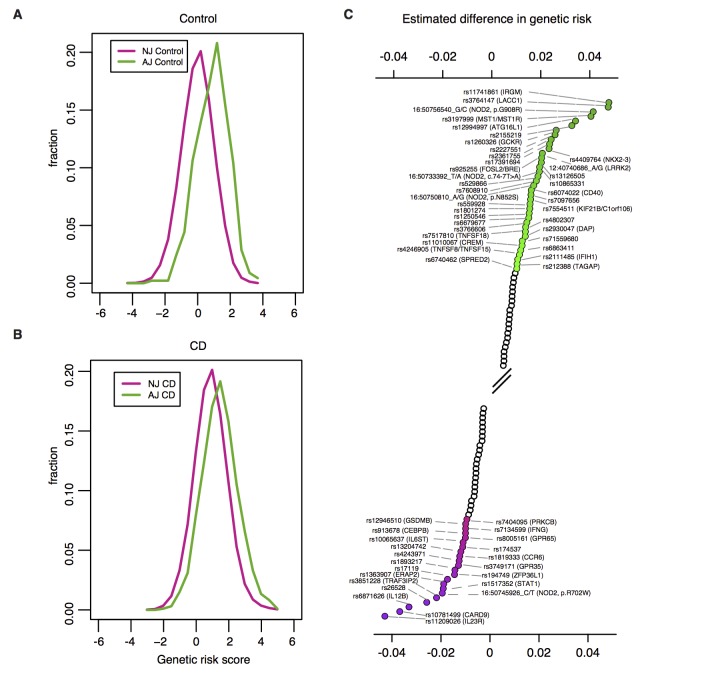
As part of a broader collaborative network of exome sequencing studies, we developed a jointly called data set of 5,685 Ashkenazi Jewish exomes. We make publicly available a resource of site and allele frequencies, which should serve as a reference for medical genetics in the Ashkenazim (hosted in part at https://ibd.broadinstitute.org, also available in gnomAD at http://gnomad.broadinstitute.org). We estimate that 34% of protein-coding alleles present in the Ashkenazi Jewish population at frequencies greater than 0.2% are significantly more frequent (mean 15-fold) than their maximum frequency observed in other reference populations. Arising via a well-described founder effect approximately 30 generations ago, this catalog of enriched alleles can contribute to differences in genetic risk and overall prevalence of diseases between populations. As validation we document 148 AJ enriched protein-altering alleles that overlap with "pathogenic" ClinVar alleles (table available at https://github.com/macarthur-lab/clinvar/blob/master/output/clinvar.tsv), including those that account for 10-100 fold differences in prevalence between AJ and non-AJ populations of some rare diseases, especially recessive conditions, including Gaucher disease (GBA, p.Asn409Ser, 8-fold enrichment); Canavan disease (ASPA, p.Glu285Ala, 12-fold enrichment); and Tay-Sachs disease (HEXA, c.1421+1G>C, 27-fold enrichment; p.Tyr427IlefsTer5, 12-fold enrichment). We next sought to use this catalog, of well-established relevance to Mendelian disease, to explore Crohn's disease, a common disease with an estimated two to four-fold excess prevalence in AJ. We specifically attempt to evaluate whether strong acting rare alleles, particularly protein-truncating or otherwise large effect-size alleles, enriched by the same founder-effect, contribute excess genetic risk to Crohn's disease in AJ, and find that ten rare genetic risk factors in NOD2 and LRRK2 are enriched in AJ (p < 0.005), including several novel contributing alleles, show evidence of association to CD. Independently, we find that genomewide common variant risk defined by GWAS shows a strong difference between AJ and non-AJ European control population samples (0.97 s.d. higher, p<10-16). Taken together, the results suggest coordinated selection in AJ population for higher CD risk alleles in general. The results and approach illustrate the value of exome sequencing data in case-control studies along with reference data sets like ExAC (sites VCF available via FTP at ftp.broadinstitute.org/pub/ExAC_release/release0.3/) to pinpoint genetic variation that contributes to variable disease predisposition across populations.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Ostrer H. & Skorecki K. The population genetics of the Jewish people. Hum. Genet. 132, 119–127 (2012). doi: 10.1007/s00439-012-1235-6 - DOI - PMC - PubMed
-
- Moltke I., Grarup N., Jørgensen M. E., Bjerregaard P., Treebak J.T., Fumagalli M., et al. A common Greenlandic TBC1D4 variant confers muscle insulin resistance and type 2 diabetes. Nature 512, 190–193 (2014). doi: 10.1038/nature13425 - DOI - PubMed
-
- Lim E. T., Würtz P., Havulinna A. S., Palta P., Tukiainen T., Rehnström K., et al. Distribution and medical impact of loss-of-function variants in the Finnish founder population. PLoS Genet. 10, e1004494 (2014). doi: 10.1371/journal.pgen.1004494 - DOI - PMC - PubMed
-
- Zuk O., Schaffner S. F., Samocha K., Do R., Hechter E., Kathiresan S., et al. Searching for missing heritability: designing rare variant association studies. Proc. Natl. Acad. Sci. U. S. A. 111, E455–64 (2014). doi: 10.1073/pnas.1322563111 - DOI - PMC - PubMed
-
- Bahcall O. & Orli B. Rare variant association studies. Nat. Genet. 46, 219–219 (2014).
Publication types
MeSH terms
Grants and funding
- U54 HG003067/HG/NHGRI NIH HHS/United States
- P30 DK043351/DK/NIDDK NIH HHS/United States
- U24 DK062429/DK/NIDDK NIH HHS/United States
- K01 DK114379/DK/NIDDK NIH HHS/United States
- U01 DK062422/DK/NIDDK NIH HHS/United States
- U01 DK062423/DK/NIDDK NIH HHS/United States
- P30 DK089502/DK/NIDDK NIH HHS/United States
- U01 DK062432/DK/NIDDK NIH HHS/United States
- P01 DK046763/DK/NIDDK NIH HHS/United States
- 5 U54 HG003067-13 /NH/NIH HHS/United States
- U01 DK062420/DK/NIDDK NIH HHS/United States
- U01 DK062431/DK/NIDDK NIH HHS/United States
- R01 DK092235/DK/NIDDK NIH HHS/United States
- R01 DK097485/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
