

Gestational Age and Maternal Serum 25-hydroxyvitamin D Concentration Interact to Affect the 24,25-dihydroxyvitamin D Concentration in Pregnant Adolescents
- PMID: 29796622
- PMCID: PMC6014295
- DOI: 10.1093/jn/nxy043
Gestational Age and Maternal Serum 25-hydroxyvitamin D Concentration Interact to Affect the 24,25-dihydroxyvitamin D Concentration in Pregnant Adolescents
Abstract
Background: Interpretation of serum vitamin D biomarkers across pregnancy is complex due to limited understanding of pregnancy adaptations in vitamin D metabolism. During pregnancy, both gestational age and serum 25-hydroxyvitamin D [25(OH)D] concentrations may influence the concentrations of 1,25-dihydroxyvitamin D [1,25(OH)2D], 24,25-dihydroxyvitamin D [24,25(OH)2D], and parathyroid hormone (PTH).
Objective: We aimed to identify predictors of change in serum 25(OH)D across gestation in pregnant adolescents and to assess the contribution made by cholecalciferol (vitamin D3) supplementation. We sought to determine whether gestational age and 25(OH)D concentration interacted to affect serum 1,25(OH)2D, 24,25(OH)2D, or PTH.
Methods: Pregnant adolescents (n = 78, 59% African American, mean ± SD age: 17 ± 1 y) living in Rochester, NY (latitude 43°N) were supplemented with 200 IU or 2000 IU vitamin D3/d and allowed to continue their daily prenatal supplement that contained 400 IU vitamin D3. Serum was collected at study entry (18 ± 5 wk of gestation), halfway through study participation, and at delivery (40 ± 2 wk). Serum concentrations of the biochemical markers were modeled with linear mixed-effects regression models.
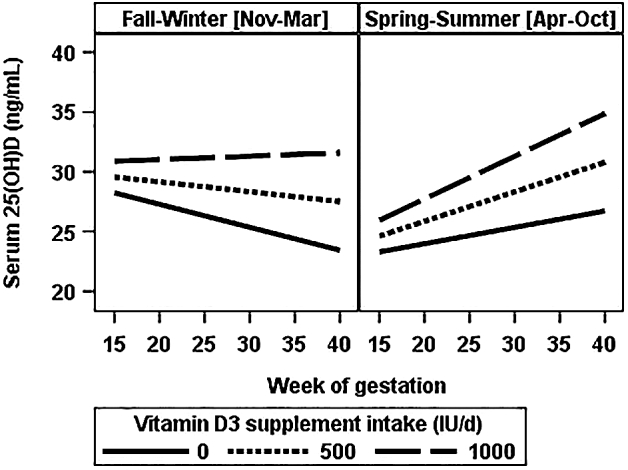
Results: Vitamin D3 supplement intake and season of delivery determined change in 25(OH)D across pregnancy. Fall-winter delivery was associated with a decline in 25(OH)D unless vitamin D3 supplement intake was >872 IU/d. The interaction of gestational age and 25(OH)D affected 24,25(OH)2D concentrations. For a given 25(OH)D concentration, model-predicted serum 24,25(OH)2D increased across gestation except when 25(OH)D was <13 ng/mL. Below this threshold, 24,25(OH)2D was predicted to decline over time. Mean serum 1,25(OH)2D was elevated (>100 pg/mL) throughout the study.
Conclusion: Our results suggest that when maternal serum 25(OH)D was low, its catabolism into 24,25(OH)2D decreased or remained stable as pregnancy progressed in order to maintain persistently elevated serum 1,25(OH)2D. Furthermore, in adolescents living at latitude 43°N, standard prenatal supplementation did not prevent a seasonal decline in 25(OH)D during pregnancy. This study was registered at clinicaltrials.gov as NCT01815047.
Figures

References
-
- Olausson H, Goldberg GR, Laskey MA, Schoenmakers I, Jarjou LM, Prentice A. Calcium economy in human pregnancy and lactation. Nutrition Res Rev 2012;25:40–67. - PubMed
-
- Baxter-Jones AD, Faulkner RA, Forwood MR, Mirwald RL, Bailey DA. Bone mineral accrual from 8 to 30 years of age: an estimation of peak bone mass. J Bone Miner Res 2011;26:1729–39. - PubMed
-
- Berner LA, Keast DR, Bailey RL, Dwyer JT. Fortified foods are major contributors to nutrient intakes in diets of US children and adolescents. J Acad Nutr Diet 2014;114:1009–22.e8. - PubMed
-
- Brannon PM, Picciano MF. Vitamin D in pregnancy and lactation in humans. Annu Rev Nutr 2011;31:89–115. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
