

Successful repair using thymus pedicle flap for tracheoesophageal fistula: a case report
- PMID: 29796790
- PMCID: PMC5966367
- DOI: 10.1186/s40792-018-0458-8
Successful repair using thymus pedicle flap for tracheoesophageal fistula: a case report
Abstract
Background: Treatment for tracheoesophageal fistula (TEF), a life-threatening complication after esophagectomy, is challenging.
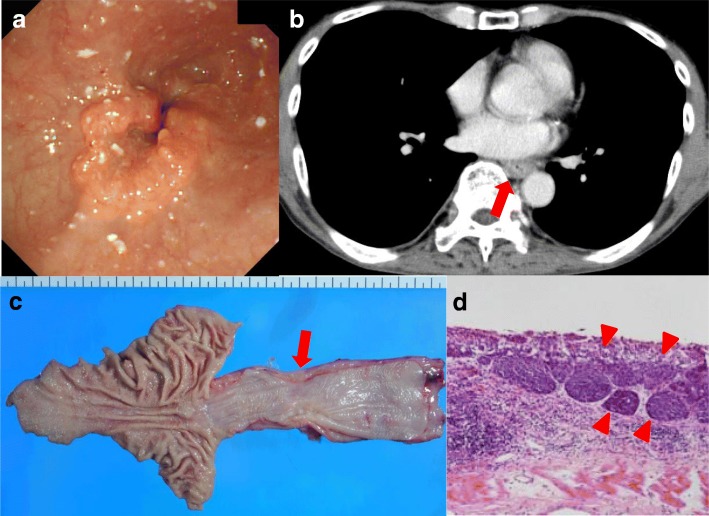
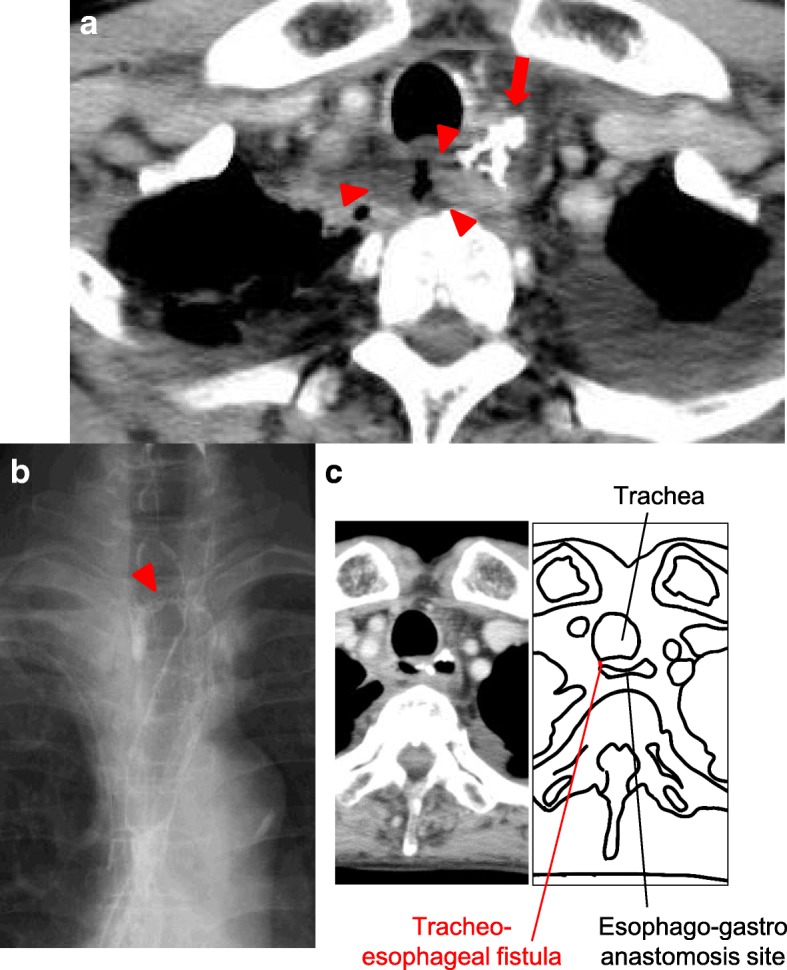
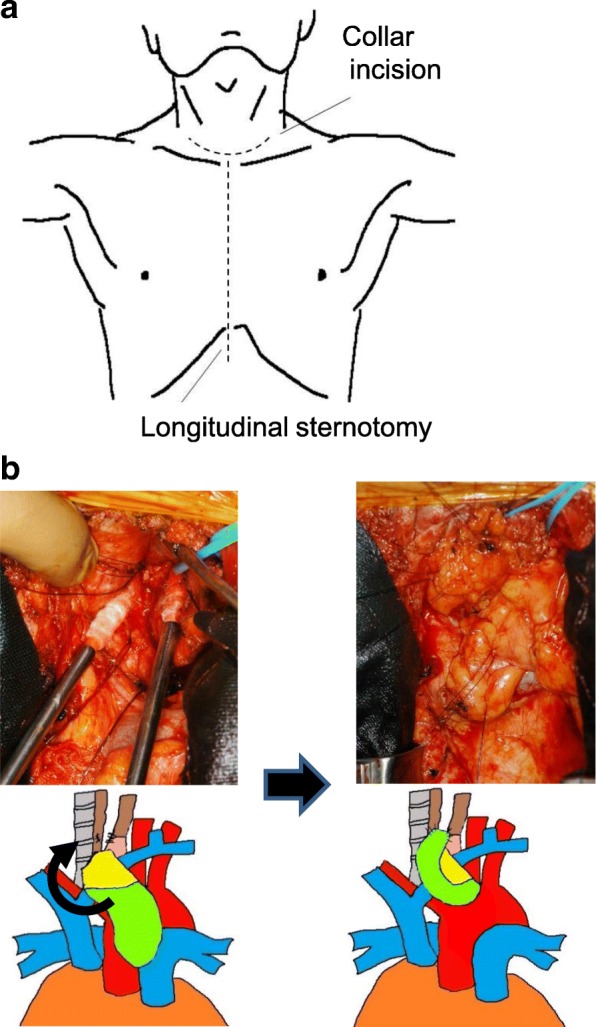
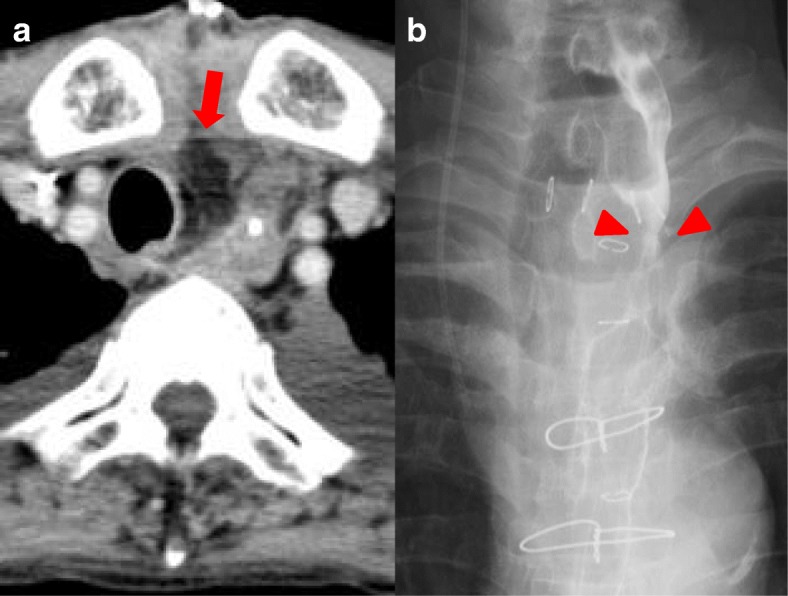
Case presentation: A 75-year-old man with thoracic esophageal cancer underwent subtotal esophagectomy and gastric tube reconstruction through the post-mediastinal root after neoadjuvant chemotherapy. Owing to postoperative anastomotic leakage, an abscess formed at the anastomotic region. Sustained inflammation from the abscess caused refractory TEF between the esophagogastric anastomotic site and membrane of the trachea, and several conservative therapies for TEF failed. Hence, the patient underwent surgery including division of the fistula, direct suturing of the leakage sites, and reinforcement with the flap of the thymus pedicle. As a result, the abscess and TEF disappeared after surgery and the patient was immediately administered an oral diet and discharged home 103 days after initial surgery.
Conclusions: Although pedicle flaps for the reinforcement of TEF are usually obtained from muscle or pericardium, these flaps need enough lengths to overcome moving distance. We are the first in the existing literature to have successfully treated TEF with surgical repair using a thymus flap located close to TEF. The thymus pedicle might be another candidate for the reinforcement flap in TEF.
Keywords: Esophageal cancer; Post-operative complication; Thymus pedicle flap; Tracheoesophageal fistula.
Conflict of interest statement
Ethics approval and consent to participate
Written informed consent was obtained from the patient for publication of this case report and its accompanying images. A copy of the written consent is available for review by the editor-in-chief of this journal on request.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
