

Steroid Hormone Vitamin D: Implications for Cardiovascular Disease
- PMID: 29798901
- PMCID: PMC6122607
- DOI: 10.1161/CIRCRESAHA.118.311585
Steroid Hormone Vitamin D: Implications for Cardiovascular Disease
Abstract
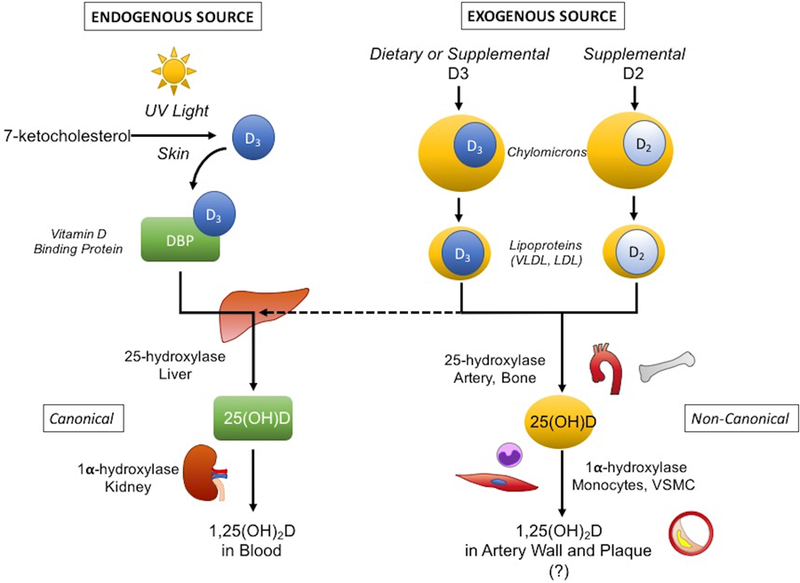
Understanding of vitamin D physiology is important because about half of the population is being diagnosed with deficiency and treated with supplements. Clinical guidelines were developed based on observational studies showing an association between low serum levels and increased cardiovascular risk. However, new randomized controlled trials have failed to confirm any cardiovascular benefit from supplementation in the general population. A major concern is that excess vitamin D is known to cause calcific vasculopathy and valvulopathy in animal models. For decades, administration of vitamin D has been used in rodents as a reliable experimental model of vascular calcification. Technically, vitamin D is a misnomer. It is not a true vitamin because it can be synthesized endogenously through ultraviolet exposure of the skin. It is a steroid hormone that comes in 3 forms that are sequential metabolites produced by hydroxylases. As a fat-soluble hormone, the vitamin D-hormone metabolites must have special mechanisms for delivery in the aqueous bloodstream. Importantly, endogenously synthesized forms are carried by a binding protein, whereas dietary forms are carried within lipoprotein particles. This may result in distinct biodistributions for sunlight-derived versus supplement-derived vitamin D hormones. Because the cardiovascular effects of vitamin D hormones are not straightforward, both toxic and beneficial effects may result from current recommendations.
Keywords: cardiovascular diseases; cholecalciferol; lipoproteins; vascular calcification; vitamin D.
© 2018 American Heart Association, Inc.
Figures

References
-
- Committee IoM. In: Ross AC, Taylor CL, Yaktine AL, Del Valle HB, eds. Dietary reference intakes for calcium and vitamin d Washington (DC: ); 2011. - PubMed
-
- Towler DA. Calciotropic hormones and arterial physiology: “D”-lightful insights. J Am Soc Nephrol 2007;18:369–373 - PubMed
-
- Fraser DR. Vitamin d. Lancet 1995;345:104–107 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
