

Grading of carotid artery stenosis with computed tomography angiography: whether to use the narrowest diameter or the cross-sectional area
- PMID: 29799095
- PMCID: PMC6108978
- DOI: 10.1007/s13244-018-0622-5
Grading of carotid artery stenosis with computed tomography angiography: whether to use the narrowest diameter or the cross-sectional area
Abstract
Objectives: To compare the estimation of carotid artery stenosis by computed tomography angiography (CTA) based on cross-sectional area versus the smallest diameter measurement, and test the accuracy of both CTA measurements using color Doppler ultrasonography (CDUS) as a reference method.
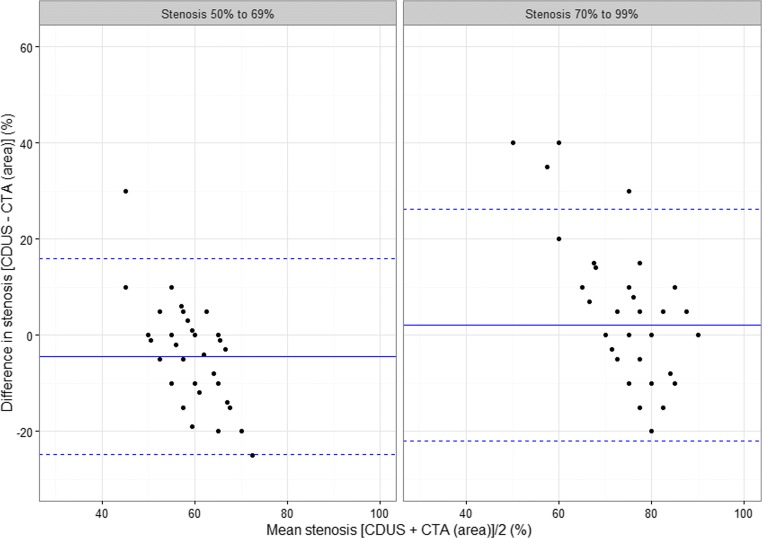
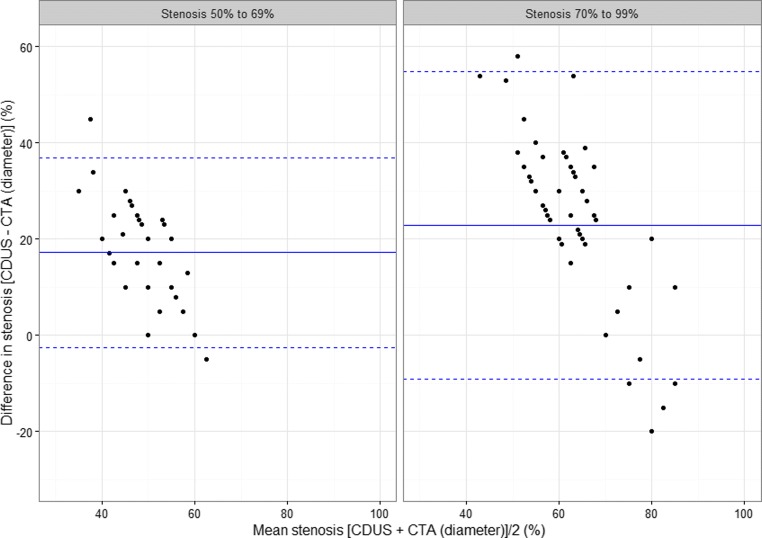
Methods: For 113 carotid arteries with stenosis ≥50% we analysed the differences in the estimated stenosis level between both CTA methods and CDUS using the Bland-Altman approach. Further, we calculated sensitivity, specificity and plotted receiver operating characteristic (ROC) curves for both CTA methods.
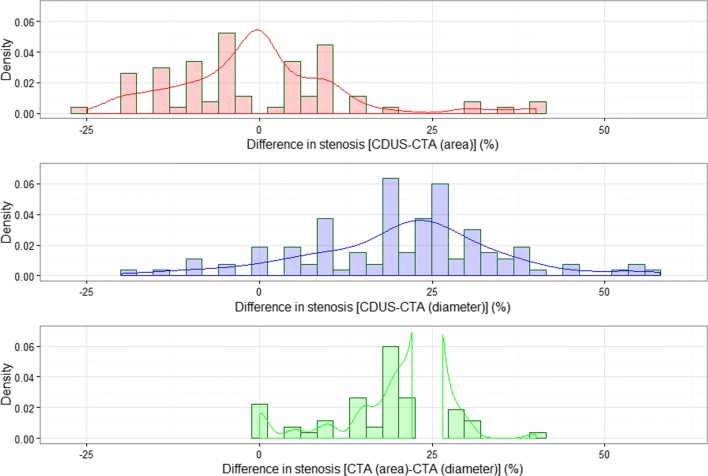
Results: The mean difference between CDUS and CTA (area) measurements was -0.4% (p = 0.68); between CDUS and CTA (diameter), 20.7% (p < 0.001); and between CTA (area) and CTA (diameter), 21.2% (p < 0.001). Sensitivity and specificity for the CTA (area) method were 81% and 77%, and for CTA (diameter) were 23% and 100%. The area under the curve (AUC) for CTA (diameter) was 0.62 (0.57, 0.66), and for CTA (area) 0.79 (0.71-0.87). The equality test for the two AUCs was <0.0001.
Conclusions: CTA (diameter)-based measurements significantly underestimated the degree of carotid stenosis. We recommend the CTA (area) method because of its higher predictive power for a correct stenosis classification and a lack of significant difference in the estimated stenosis level, compared to CDUS.
Main messages: • Cross-sectional area measurement considers asymmetric shape of the residual vessel lumen. • CTA (diameter) method on average significantly underestimates the true level of stenosis. • CTA (area) method correctly classifies vessels needing surgical intervention.
Keywords: Atherosclerosis; CT angiography; Carotid artery stenosis; Color Doppler ultrasonography; Medical imaging.
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources
