

An analysis of surgical and anaesthetic factors affecting skin graft viability in patients admitted to a Burns Intensive Care Unit
- PMID: 29799557
- PMCID: PMC5965314
- DOI: 10.1177/2059513116642089
An analysis of surgical and anaesthetic factors affecting skin graft viability in patients admitted to a Burns Intensive Care Unit
Abstract
Objectives: Skin graft failure is a recognised complication in the treatment of major burns. Little research to date has analysed the impact of the complex physiological management of burns patients on the success of skin grafting. We analysed surgical and anaesthetic variables to identify factors contributing to graft failure.
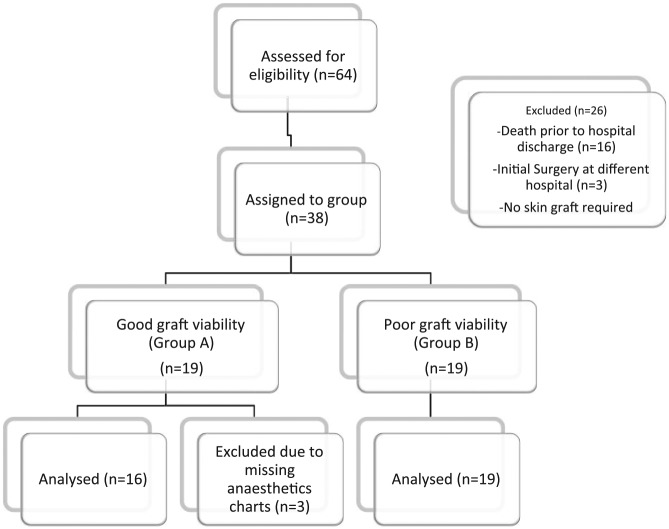
Methods: Inclusion criteria were admission to our Burns Intensive Care Unit (BICU) between January 2009 and October 2013 with a major burn. After exclusion for death before hospital discharge or prior skin graft at a different hospital, 35 patients remained and were divided into those with successful autografts (n=16) and those with a failed autograft (n=19). For the purposes of this study, we defined poor autograft viability as requiring at least one additional skin graft to the same site. Logistic regression of variables was performed using SPSS (Version 22.0 IBMTM).
Results: Age, Sex, %Total Burn Surface Area or Belgian Outcome Burns Injury score did not significantly differ between groups. No differences were found in any surgical factor at logistic regression (graft site, harvest site, infection etc.). When all operations were analysed, the use of colloids was found to be significantly associated with graft failure (p=0.035, CI 95%) and this remained significant when only split thickness skin grafts (STSGs) and debridement operations were included (p=0.034, CI 95%). No differences were found in crystalloid use, intraoperative temperature, pre-operative haemoglobin and blood products or vasopressor use.
Conclusions: This analysis highlights an independent association between colloids and graft failure which has not been previously documented.
Keywords: Graft failure; anaesthetic management; burns; burns intensive care unit; colloids; skin graft.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The anaesthetics data were originally presented by CE Isitt and KA McCloskey at ISICEM conference in Brussels, Belgium in March 2015 and the surgical data were presented at the Nordic Burn meeting in Linkoping, Sweden in May 2014 by A Caballo.
Figures
Similar articles
-
[Analysis of reasons for failure of Meek micro-skin grafting in children with severe burn and treatment measures].Zhonghua Shao Shang Za Zhi. 2019 Jul 20;35(7):525-531. doi: 10.3760/cma.j.issn.1009-2587.2019.07.009. Zhonghua Shao Shang Za Zhi. 2019. PMID: 31357823 Chinese.
-
Factors affecting success of split-thickness skin grafts in the modern burn unit.J Trauma. 2003 Mar;54(3):562-8. doi: 10.1097/01.TA.0000053246.04307.2E. J Trauma. 2003. PMID: 12634539
-
Revised Baux Score and updated Charlson comorbidity index are independently associated with mortality in burns intensive care patients.Burns. 2015 Nov;41(7):1420-7. doi: 10.1016/j.burns.2015.06.009. Epub 2015 Jul 14. Burns. 2015. PMID: 26187055
-
Intermediate Skin Substitutes Are Unnecessary in Small (<10% TBSA) Burns.J Burn Care Res. 2020 Sep 23;41(5):926-928. doi: 10.1093/jbcr/iraa077. J Burn Care Res. 2020. PMID: 32485731
-
A review of negative-pressure wound therapy in the management of burn wounds.Burns. 2016 Dec;42(8):1623-1633. doi: 10.1016/j.burns.2016.06.011. Epub 2016 Jul 1. Burns. 2016. PMID: 27378361 Review.
Cited by
-
Scars, Burns and Healing.Scars Burn Heal. 2016 Apr 22;2:2059513116642395. doi: 10.1177/2059513116642395. eCollection 2016 Jan-Dec. Scars Burn Heal. 2016. PMID: 29799560 Free PMC article. No abstract available.
-
Colloid resuscitation in burns: controversies and perspectives.Scars Burn Heal. 2016 Apr 22;2:2059513116645224. doi: 10.1177/2059513116645224. eCollection 2016 Jan-Dec. Scars Burn Heal. 2016. PMID: 29799584 Free PMC article. No abstract available.
-
Autologous Skin Grafts, versus Tissue-engineered Skin Constructs: A Systematic Review and Meta-analysis.Plast Reconstr Surg Glob Open. 2023 Jun 27;11(6):e5100. doi: 10.1097/GOX.0000000000005100. eCollection 2023 Jun. Plast Reconstr Surg Glob Open. 2023. PMID: 37388427 Free PMC article.
-
An Open-Label Study of Low-Level Laser Therapy Followed by Autologous Fibroblast Transplantation for Healing Grade 3 Burn Wounds in Diabetic Patients.J Lasers Med Sci. 2019 Fall;10(Suppl 1):S7-S12. doi: 10.15171/jlms.2019.S2. Epub 2019 Dec 1. J Lasers Med Sci. 2019. PMID: 32021666 Free PMC article.
References
-
- Harbin KR, Norris TE. Anaesthetic management of patients with major burn injury. AANA Journal 2012; 80(6): 430–439. - PubMed
-
- Orgill DP, Ogawa RO. Current methods of burn reconstruction. Plast Reconstr Surg 2013; 131(5): 827e–836e. - PubMed
-
- Herndon DN, Tompkins RG. Support of the metabolic response to burn injury. Lancet 2004; 363: 9424. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
