

Complement-activating donor-specific anti-HLA antibodies and solid organ transplant survival: A systematic review and meta-analysis
- PMID: 29799874
- PMCID: PMC5969739
- DOI: 10.1371/journal.pmed.1002572
Complement-activating donor-specific anti-HLA antibodies and solid organ transplant survival: A systematic review and meta-analysis
Erratum in
-
Correction: Complement-activating donor-specific anti-HLA antibodies and solid organ transplant survival: A systematic review and meta-analysis.PLoS Med. 2018 Jul 27;15(7):e1002637. doi: 10.1371/journal.pmed.1002637. eCollection 2018 Jul. PLoS Med. 2018. PMID: 30052664 Free PMC article.
Abstract
Background: Anti-human leukocyte antigen donor-specific antibodies (anti-HLA DSAs) are recognized as a major barrier to patients' access to organ transplantation and the major cause of graft failure. The capacity of circulating anti-HLA DSAs to activate complement has been suggested as a potential biomarker for optimizing graft allocation and improving the rate of successful transplantations.
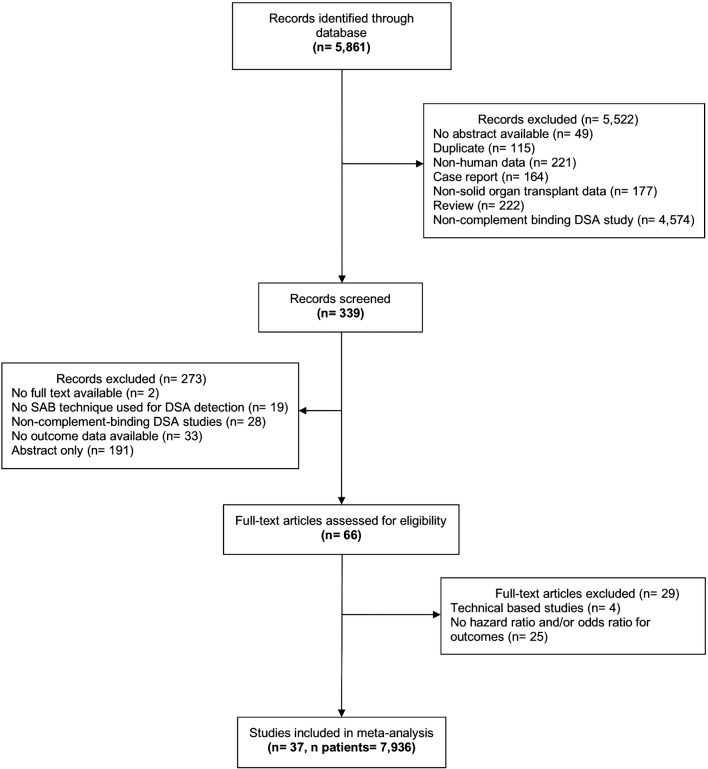
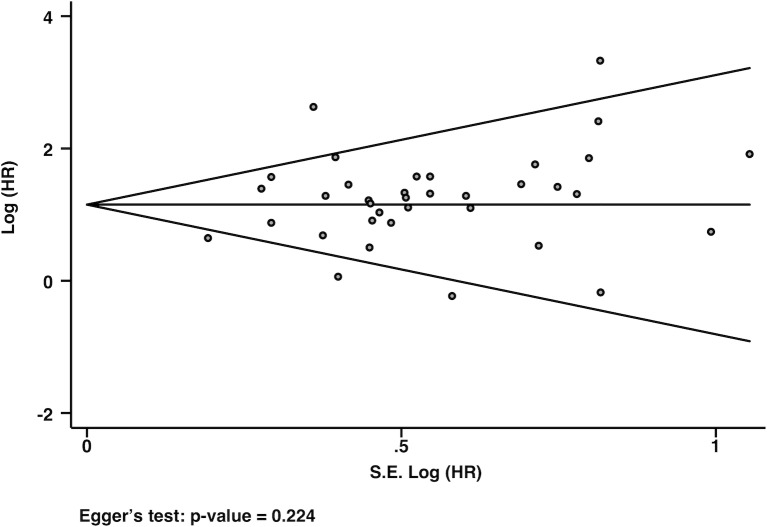
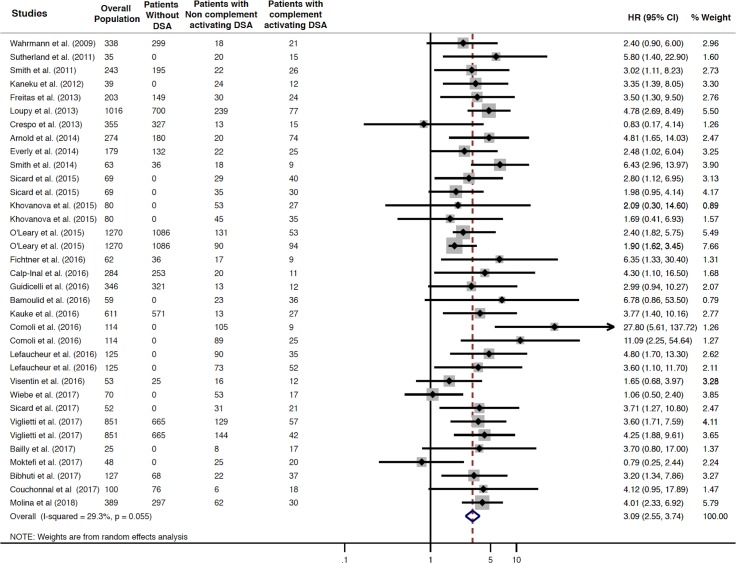
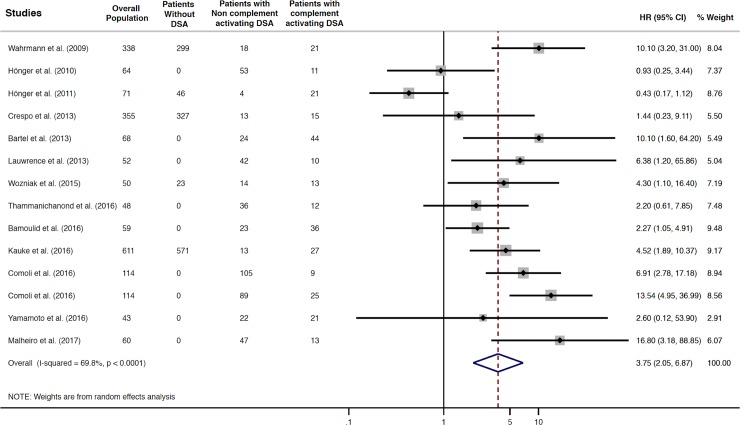
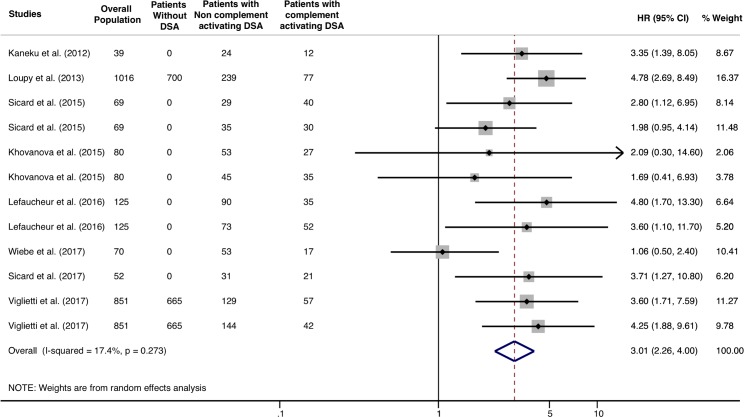
Methods and findings: To address the clinical relevance of complement-activating anti-HLA DSAs across all solid organ transplant patients, we performed a meta-analysis of their association with transplant outcome through a systematic review, from inception to January 31, 2018. The primary outcome was allograft loss, and the secondary outcome was allograft rejection. A comprehensive search strategy was conducted through several databases (Medline, Embase, Cochrane, and Scopus). A total of 5,861 eligible citations were identified. A total of 37 studies were included in the meta-analysis. Studies reported on 7,936 patients, including kidney (n = 5,991), liver (n = 1,459), heart (n = 370), and lung recipients (n = 116). Solid organ transplant recipients with circulating complement-activating anti-HLA DSAs experienced an increased risk of allograft loss (pooled HR 3.09; 95% CI 2.55-3.74, P = 0.001; I2 = 29.3%), and allograft rejection (pooled HR 3.75; 95% CI: 2.05-6.87, P = 0.001; I2 = 69.8%) compared to patients without complement-activating anti-HLA DSAs. The association between circulating complement-activating anti-HLA DSAs and allograft failure was consistent across all subgroups and sensitivity analyses. Limitations of the study are the observational and retrospective design of almost all included studies, the higher proportion of kidney recipients compared to other solid organ transplant recipients, and the inclusion of fewer studies investigating allograft rejection.
Conclusions: In this study, we found that circulating complement-activating anti-HLA DSAs had a significant deleterious impact on solid organ transplant survival and risk of rejection. The detection of complement-activating anti-HLA DSAs may add value at an individual patient level for noninvasive biomarker-guided risk stratification.
Trial registration: National Clinical Trial protocol ID: NCT03438058.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: AMJ declares Speaker Bureau with Honoraria for ThermoFisher-One Lambda Corporation. ThermoFisher-One Lambda Corporation is involved in the manufacture of C1q anti-HLA antibody test. JK has received research grants and/or research support from Novartis, CareDx, and TransMedics.
Figures
References
-
- Port FK, Wolfe RA, Mauger EA, Berling DP, Jiang K. Comparison of survival probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA. 1993;270: 1339–1343. - PubMed
-
- Stehlik J, Edwards LB, Kucheryavaya AY, Benden C, Christie JD, Dobbels F, et al. The Registry of the International Society for Heart and Lung Transplantation: Twenty–eighth Adult Heart Transplant Report––2011. J Heart Lung Transplant. 2011;30: 1078–1094. doi: 10.1016/j.healun.2011.08.003 - DOI - PubMed
-
- Organ Procurement and Transplantation Network: Scientific registry of transplant recipients. [Cited 1 January 2018]. Available from: http://optn.transplant.hrsa.gov/data/. - PubMed
-
- Eurotransplant Annual Report. [Cited 1 January 2018]. Available from: https://www.eurotransplant.org/cms/index.php?page=annual_reports.
-
- Nankivell BJ, Alexander SI. Rejection of the kidney allograft. N Engl J Med. 2010;363: 1451–1462. doi: 10.1056/NEJMra0902927 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
