

Trends in Platelet Adenosine Diphosphate P2Y12 Receptor Inhibitor Use and Adherence Among Antiplatelet-Naive Patients After Percutaneous Coronary Intervention, 2008-2016
- PMID: 29799992
- PMCID: PMC6145718
- DOI: 10.1001/jamainternmed.2018.0783
Trends in Platelet Adenosine Diphosphate P2Y12 Receptor Inhibitor Use and Adherence Among Antiplatelet-Naive Patients After Percutaneous Coronary Intervention, 2008-2016
Abstract
Importance: Current guidelines recommend prasugrel hydrochloride and ticagrelor hydrochloride as preferred therapies for patients with acute coronary syndrome (ACS) treated with percutaneous coronary intervention (PCI). However, it is not well known how frequently these newer agents are being used in clinical practice or how adherence varies among the platelet adenosine diphosphate P2Y12 receptor (P2Y12) inhibitors.
Objectives: To determine trends in use of the different P2Y12 inhibitors in patients who underwent PCI from 2008 to 2016 in a large cohort of commercially insured patients and differences in patient adherence and costs among the P2Y12 inhibitors.
Design, setting, and participants: A retrospective cohort study used administrative claims from a large US national insurer (ie, UnitedHealthcare) from January 1, 2008, to December 1, 2016, comprising patients aged 18 to 64 years hospitalized for PCI who had not received a P2Y12 inhibitor for 90 days preceding PCI. The P2Y12 inhibitor filled within 30 days of discharge was identified from pharmacy claims.
Main outcomes and measures: Proportion of patients filling prescriptions for P2Y12 inhibitors within 30 days of discharge by year, as well as medication possession ratios (MPRs) and total P2Y12 inhibitor copayments at 6 and 12 months for patients who received drug-eluting stents.
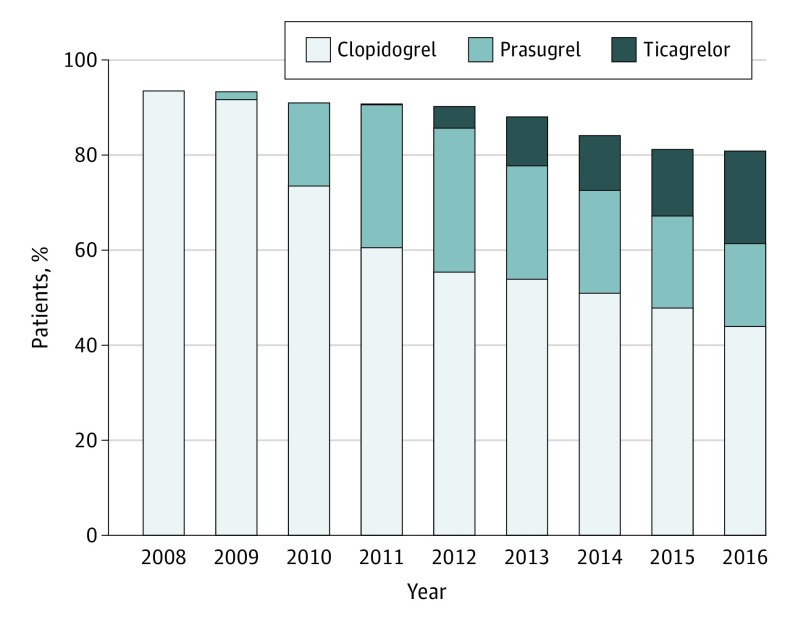
Results: A total of 55 340 patients (12 754 [23.0%] women; mean [SD] age, 54.4 [7.1] years) who underwent PCI were included in this study. In 2008, 7667 (93.6%) patients filled a prescription for clopidogrel bisulfate and 521 (6.4%) filled no P2Y12 inhibitor prescription within 30 days of hospitalization. In 2016, 2406 (44.0%) patients filled clopidogrel prescriptions, 2015 (36.9%) filled either prasugrel or ticagrelor prescriptions, and 1045 (19.1%) patients filled no P2Y12 inhibitor prescription within 30 days of hospitalization. At 6 months, mean MPRs for patients who received a drug-eluting stent filling clopidogrel, prasugrel, and ticagrelor prescriptions were 0.85 (interquartile range [IQR], 0.82-1.00), 0.79 (IQR, 0.66-1.00), and 0.76 (IQR, 0.66-0.98) (P < .001), respectively; mean copayments for a 6 months' supply were $132 (IQR, $47-$203), $287 (IQR, $152-$389), and $265 (IQR, $53-$387) (P < .001), respectively. At 12 months, mean MPRs for clopidogrel, prasugrel, and ticagrelor were 0.76 (IQR, 0.58-0.99), 0.71 (IQR, 0.49-0.98), and 0.68 (IQR, 0.41-0.94) (P < .001), respectively; mean total copayments were $251 (IQR, $100-$371), $556 (IQR, $348-$730), and $557 (IQR, $233-$744) (P < .001), respectively.
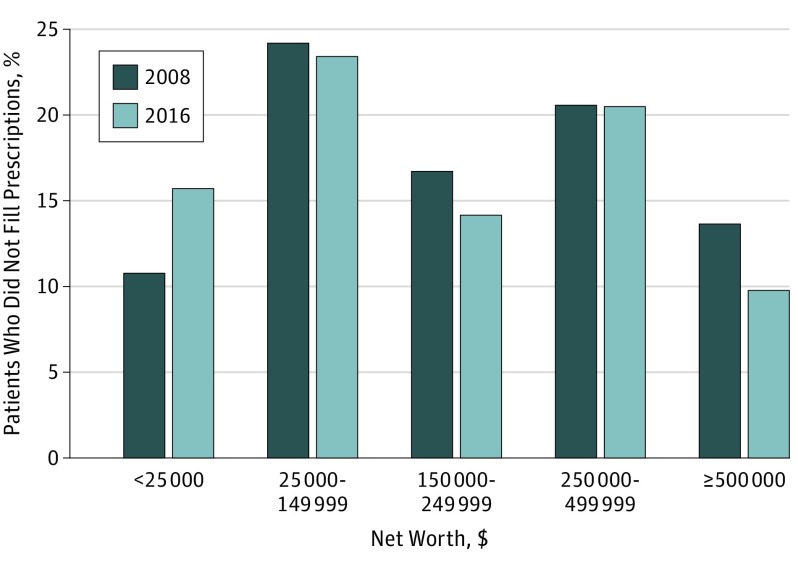
Conclusions and relevance: Between 2008 and 2016, increased use of prasugrel and ticagrelor was accompanied by increased nonfilling of prescriptions for P2Y12 inhibitors within 30 days of discharge. Prasugrel and ticagrelor had higher patient costs and lower adherence in the year following PCI compared with clopidogrel. The introduction of newer, more expensive P2Y12 inhibitors was associated with lower adherence to these therapies.
Conflict of interest statement
Figures
Comment in
-
A Call for a Systems-Thinking Approach to Medication Adherence: Stop Blaming the Patient.JAMA Intern Med. 2018 Jul 1;178(7):950-951. doi: 10.1001/jamainternmed.2018.0790. JAMA Intern Med. 2018. PMID: 29799994 No abstract available.
References
-
- Wiviott SD, Braunwald E, McCabe CH, et al. ; TRITON-TIMI 38 Investigators . Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357(20):2001-2015. - PubMed
-
- Wallentin L, Becker RC, Budaj A, et al. ; PLATO Investigators . Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009;361(11):1045-1057. - PubMed
-
- Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: an update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients With Non–ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. Circulation. 2016;134(10):e123-e155. - PubMed
-
- Karve AM, Seth M, Sharma M, et al. Contemporary use of ticagrelor in interventional practice (from Blue Cross Blue Shield of Michigan Cardiovascular Consortium). Am J Cardiol. 2015;115(11):1502-1506. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
