

Aldosterone Antagonist Therapy and Mortality in Patients With ST-Segment Elevation Myocardial Infarction Without Heart Failure: A Systematic Review and Meta-analysis
- PMID: 29799995
- PMCID: PMC6145720
- DOI: 10.1001/jamainternmed.2018.0850
Aldosterone Antagonist Therapy and Mortality in Patients With ST-Segment Elevation Myocardial Infarction Without Heart Failure: A Systematic Review and Meta-analysis
Abstract
Importance: Treatment with aldosterone antagonists is recommended and has been shown to have beneficial effects in patients with ST-segment elevation myocardial infarction (STEMI) and left ventricular ejection fraction (LVEF) less than 40%. However, the role of aldosterone antagonists in patients with ejection fraction greater than 40% or without congestive heart failure is not well known.
Objectives: To perform a systematic review and meta-analysis using standard techniques to determine the role of therapy with aldosterone antagonists in this patient population.
Data sources: PubMed, Embase, CINAHL, and Cochrane Central databases were searched and a manual search for relevant references from the selected articles and published reviews was performed from database inception through June 2017.
Study selection: Randomized clinical trials that evaluated treatment with aldosterone antagonists in patients with STEMI without clinical heart failure or LVEF greater than 40% were included.
Data extraction and synthesis: Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines were used to conduct and report the meta-analysis, which used a random-effects model. Two investigators independently performed the database search and agreed on the final study selection. A manual search was performed for relevant references from the selected articles and published reviews.
Main outcomes and measures: The outcomes analyzed were mortality, new congestive heart failure, recurrent myocardial infarction, ventricular arrhythmia, and changes in LVEF, serum potassium level, and creatinine level at follow-up.
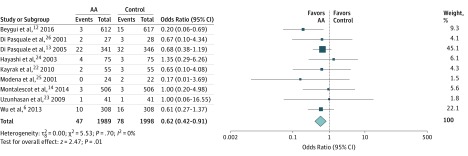
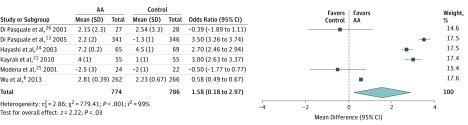
Results: In all, 10 randomized clinical trials with a total of 4147 unique patients were included in the meta-analysis. In patients who presented with STEMI without heart failure, treatment with aldosterone antagonists compared with control was associated with lower risk of mortality (2.4% vs 3.9%; odds ratio [OR], 0.62; 95% CI, 0.42-0.91; P = .01) and similar risks of myocardial infarction (1.6% vs 1.5%; OR, 1.03; 95% CI, 0.57-1.86; P = .91), new congestive heart failure (4.3% vs 5.4%; OR, 0.82; 95% CI, 0.56-1.20; P = .31), and ventricular arrhythmia (4.1% vs 5.1%; OR, 0.76; 95% CI, 0.45-1.31; P = .33). Similarly, treatment with aldosterone antagonists compared with control was associated with a small yet significant increase in LVEF (mean difference, 1.58%; 95% CI, 0.18%-2.97%; P = .03), a small increase in serum potassium level (mean difference, 0.07 mEq/L; 95% CI, 0.01-0.13 mEq/L; P = .02), and no change in serum creatinine level (standardized mean difference, 1.4; 95% CI, -0.43 to 3.24; P = .13).
Conclusions and relevance: Treatment with aldosterone antagonists is associated with a mortality benefit in patients with STEMI with LVEF greater than 40% or without heart failure.
Conflict of interest statement
Figures
Comment in
-
Mineralocorticoid Receptor Antagonists in ST-Segment Elevation Myocardial Infarction.JAMA Intern Med. 2018 Jul 1;178(7):920-921. doi: 10.1001/jamainternmed.2018.1940. JAMA Intern Med. 2018. PMID: 29799990 No abstract available.
-
Mineralocorticoid Receptor Antagonism Treatment for All Patients With ST-Segment Myocardial Infarction?JAMA Intern Med. 2018 Nov 1;178(11):1567. doi: 10.1001/jamainternmed.2018.5950. JAMA Intern Med. 2018. PMID: 30398557 No abstract available.
-
Mineralocorticoid Receptor Antagonism Treatment for All Patients With ST-Segment Myocardial Infarction?-Reply.JAMA Intern Med. 2018 Nov 1;178(11):1567-1568. doi: 10.1001/jamainternmed.2018.5964. JAMA Intern Med. 2018. PMID: 30398561 No abstract available.
Similar articles
-
Predictors of the Use of Mineralocorticoid Receptor Antagonists in Patients With Left Ventricular Dysfunction Post-ST-Segment-Elevation Myocardial Infarction.J Am Heart Assoc. 2021 Jul 20;10(14):e019167. doi: 10.1161/JAHA.120.019167. Epub 2021 Jul 6. J Am Heart Assoc. 2021. PMID: 34227405 Free PMC article.
-
Does Oral Beta-Blocker Therapy Improve Long-Term Survival in ST-Segment Elevation Myocardial Infarction With Preserved Systolic Function? A Meta-Analysis.J Cardiovasc Pharmacol Ther. 2016 May;21(3):280-5. doi: 10.1177/1074248415608011. Epub 2015 Sep 29. J Cardiovasc Pharmacol Ther. 2016. PMID: 26424094 Review.
-
Effectiveness and tolerability of administration of granulocyte colony-stimulating factor on left ventricular function in patients with myocardial infarction: a meta-analysis of randomized controlled trials.Clin Ther. 2007 Nov;29(11):2406-18. doi: 10.1016/j.clinthera.2007.11.008. Clin Ther. 2007. PMID: 18158081 Review.
-
Update on aldosterone antagonists use in heart failure with reduced left ventricular ejection fraction. Heart Failure Society of America Guidelines Committee.J Card Fail. 2012 Apr;18(4):265-81. doi: 10.1016/j.cardfail.2012.02.005. J Card Fail. 2012. PMID: 22464767
-
Efficacy of mineralocorticoid receptor antagonists in postmyocardial infarction patients with or without left ventricular dysfunction: A meta-analysis of randomized controlled trials.Medicine (Baltimore). 2018 Dec;97(51):e13690. doi: 10.1097/MD.0000000000013690. Medicine (Baltimore). 2018. PMID: 30572494 Free PMC article.
Cited by
-
Mineralocorticoid receptor antagonist pre-treatment and early post-treatment to minimize reperfusion injury after ST-elevation myocardial infarction: The MINIMIZE STEMI trial.Am Heart J. 2019 May;211:60-67. doi: 10.1016/j.ahj.2019.02.005. Epub 2019 Feb 20. Am Heart J. 2019. PMID: 30893577 Free PMC article. Clinical Trial.
-
The mineralocorticoid receptor leads to increased expression of EGFR and T-type calcium channels that support HL-1 cell hypertrophy.Sci Rep. 2021 Jun 24;11(1):13229. doi: 10.1038/s41598-021-92284-y. Sci Rep. 2021. PMID: 34168192 Free PMC article.
-
Effects of Mineralocorticoid Receptor Antagonists on Atrial Fibrillation Occurrence: A Systematic Review, Meta-Analysis, and Meta-Regression to Identify Modifying Factors.J Am Heart Assoc. 2019 Nov 19;8(22):e013267. doi: 10.1161/JAHA.119.013267. Epub 2019 Nov 12. J Am Heart Assoc. 2019. PMID: 31711383 Free PMC article.
-
Influencing factors and prognostic value of left ventricular systolic dysfunction in patients with complete occlusion of the left anterior descending artery reperfused by primary percutaneous coronary intervention.BMC Cardiovasc Disord. 2023 Jul 10;23(1):344. doi: 10.1186/s12872-023-03341-5. BMC Cardiovasc Disord. 2023. PMID: 37430213 Free PMC article.
-
Macrophage Mineralocorticoid Receptor Is a Pleiotropic Modulator of Myocardial Infarct Healing.Hypertension. 2019 Jan;73(1):102-111. doi: 10.1161/HYPERTENSIONAHA.118.12162. Hypertension. 2019. PMID: 30543467 Free PMC article.
References
-
- Ibanez B, James S, Agewall S, et al. ; ESC Scientific Document Group . 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119-177. - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, et al. ; American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions . 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61(4):e78-e140. - PubMed
-
- Pedersen F, Butrymovich V, Kelbæk H, et al. . Short- and long-term cause of death in patients treated with primary PCI for STEMI. J Am Coll Cardiol. 2014;64(20):2101-2108. - PubMed
-
- Silvestre JS, Heymes C, Oubénaïssa A, et al. . Activation of cardiac aldosterone production in rat myocardial infarction: effect of angiotensin II receptor blockade and role in cardiac fibrosis. Circulation. 1999;99(20):2694-2701. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
