

Effect of Recombinant Human Pentraxin 2 vs Placebo on Change in Forced Vital Capacity in Patients With Idiopathic Pulmonary Fibrosis: A Randomized Clinical Trial
- PMID: 29800034
- PMCID: PMC6134440
- DOI: 10.1001/jama.2018.6129
Effect of Recombinant Human Pentraxin 2 vs Placebo on Change in Forced Vital Capacity in Patients With Idiopathic Pulmonary Fibrosis: A Randomized Clinical Trial
Abstract
Importance: Idiopathic pulmonary fibrosis (IPF) is a progressive fibrotic lung disease with poor prognosis. Approved therapies do not halt disease progression.
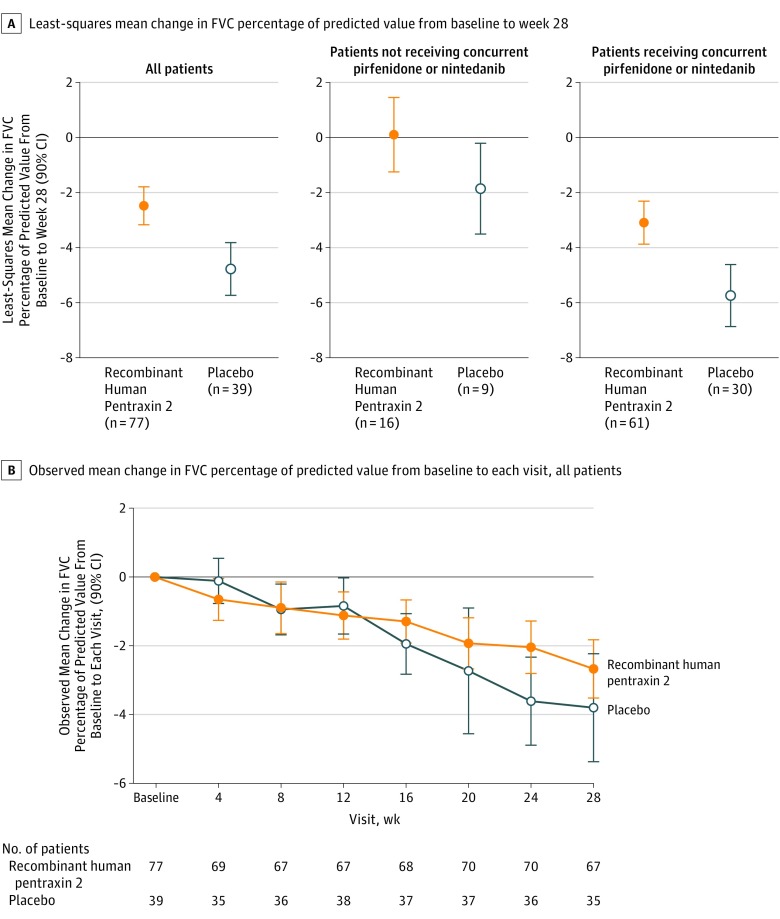
Objective: To determine the effect of recombinant human pentraxin 2 vs placebo on change from baseline to week 28 in mean forced vital capacity (FVC) percentage of predicted value.
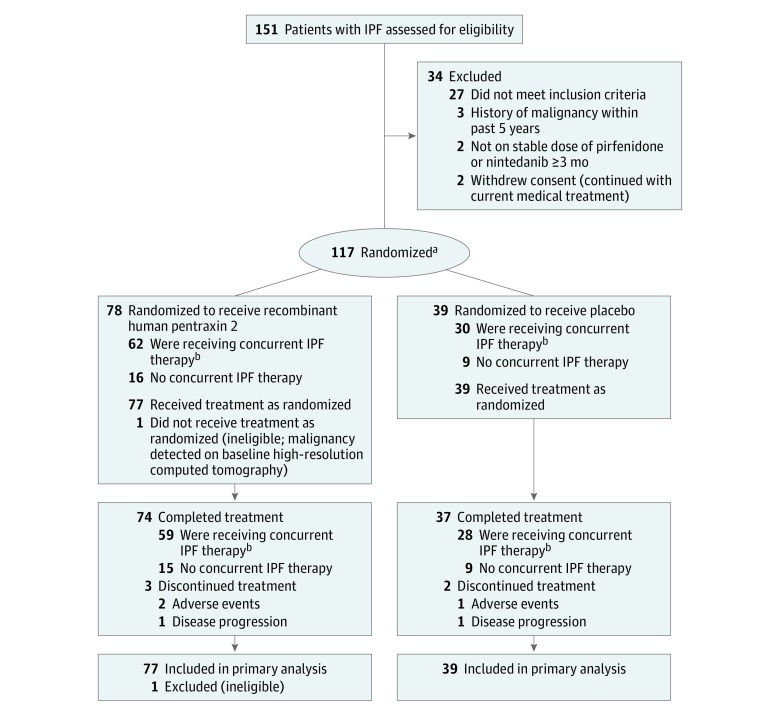
Design, setting, and participants: Phase 2, randomized, double-blind, placebo-controlled trial conducted at 18 sites in 7 countries of eligible patients with IPF (N = 117; aged 40-80 years; FVC ≥50% and ≤90% predicted; ratio of forced expiratory volume in the first second/FVC >0.70; diffusing capacity for carbon monoxide [Dlco] ≥25% and ≤90% predicted; and distance of ≥150 m on the 6-minute walk test). Study period was August 2015-May 2017.
Interventions: Patients were randomized to receive either recombinant human pentraxin 2 (10 mg/kg intravenous every 4 weeks, n = 77) or placebo (n = 39) for 24 weeks, and stratified by concurrent IPF treatment status.
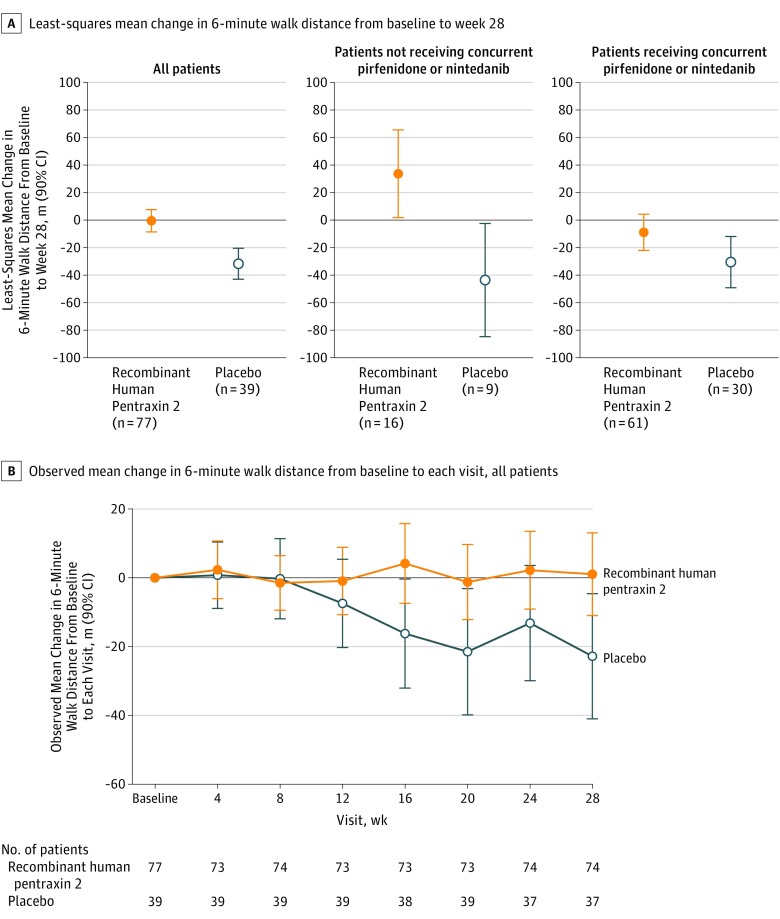
Main outcomes and measures: The primary end point was the least-squares mean change in FVC percentage of predicted value from baseline to week 28 (minimal clinically important difference, decline of 2%-6%). Secondary end points included mean change in lung volumes (total, normal, and interstitial lung abnormalities) on high-resolution computed tomography (HRCT) and 6-minute walk distance (minimal clinically important difference, 24-45 m).
Results: Of 117 randomized patients, 116 received at least 1 dose of study drug (mean age, 68.6 years; 81.0% men; mean time since IPF diagnosis, 3.8 years), and 111 (95.7%) completed the study. The least-squares mean change in FVC percentage of predicted value from baseline to week 28 in patients treated with recombinant human pentraxin 2 was -2.5 vs -4.8 for those in the placebo group (difference, +2.3 [90% CI, 1.1 to 3.5]; P = .001). No significant treatment differences were observed in total lung volume (difference, 93.5 mL [90% CI, -27.7 to 214.7]), quantitative parenchymal features on HRCT (normal lung volume difference, -1.2% [90% CI, -4.4 to 1.9]; interstitial lung abnormalities difference, 1.1% [90% CI, -2.2 to 4.3]), or measurement of Dlco (difference, -0.4 [90% CI, -2.6 to 1.7]). The change in 6-minute walk distance was -0.5 m for patients treated with recombinant human pentraxin 2 vs -31.8 m for those in the placebo group (difference, +31.3 m [90% CI, 17.4 to 45.1]; P < .001). The most common adverse events in the recombinant human pentraxin 2 vs placebo group were cough (18% vs 5%), fatigue (17% vs 10%), and nasopharyngitis (16% vs 23%).
Conclusions and relevance: In this preliminary study, recombinant human pentraxin 2 vs placebo resulted in a slower decline in lung function over 28 weeks for patients with idiopathic pulmonary fibrosis. Further research should more fully assess efficacy and safety.
Trial registration: clinicaltrials.gov Identifier: NCT02550873.
Conflict of interest statement
Figures
Comment in
-
Clinical Trials in Idiopathic Pulmonary Fibrosis in the "Posttreatment Era".JAMA. 2018 Jun 12;319(22):2275-2276. doi: 10.1001/jama.2018.6225. JAMA. 2018. PMID: 29800063 No abstract available.
References
-
- Olson AL, Swigris JJ, Lezotte DC, Norris JM, Wilson CG, Brown KK. Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003. Am J Respir Crit Care Med. 2007;176(3):277-284. - PubMed
-
- Hutchinson J, Fogarty A, Hubbard R, McKeever T. Global incidence and mortality of idiopathic pulmonary fibrosis: a systematic review. Eur Respir J. 2015;46(3):795-806. - PubMed
-
- Raghu G, Chen SY, Hou Q, Yeh WS, Collard HR. Incidence and prevalence of idiopathic pulmonary fibrosis in US adults 18-64 years old. Eur Respir J. 2016;48(1):179-186. - PubMed
-
- King TE Jr, Bradford WZ, Castro-Bernardini S, et al. ; ASCEND Study Group . A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2083-2092. - PubMed
-
- Richeldi L, du Bois RM, Raghu G, et al. ; INPULSIS Trial Investigators . Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2071-2082. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
