

Pancreatic cancer risk is modulated by inflammatory potential of diet and ABO genotype: a consortia-based evaluation and replication study
- PMID: 29800239
- PMCID: PMC6067129
- DOI: 10.1093/carcin/bgy072
Pancreatic cancer risk is modulated by inflammatory potential of diet and ABO genotype: a consortia-based evaluation and replication study
Abstract
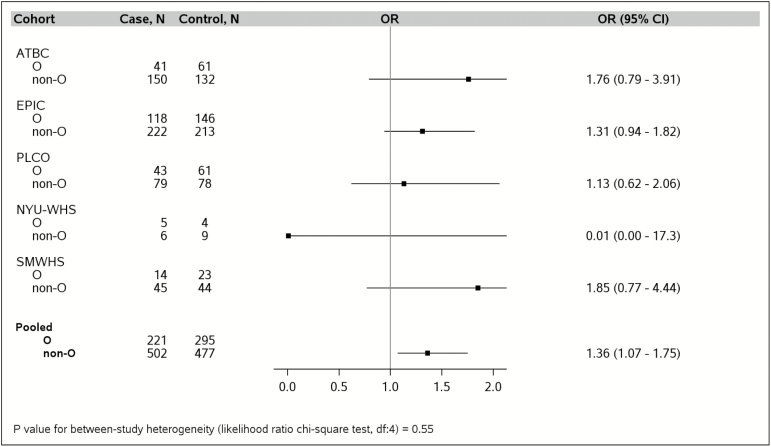
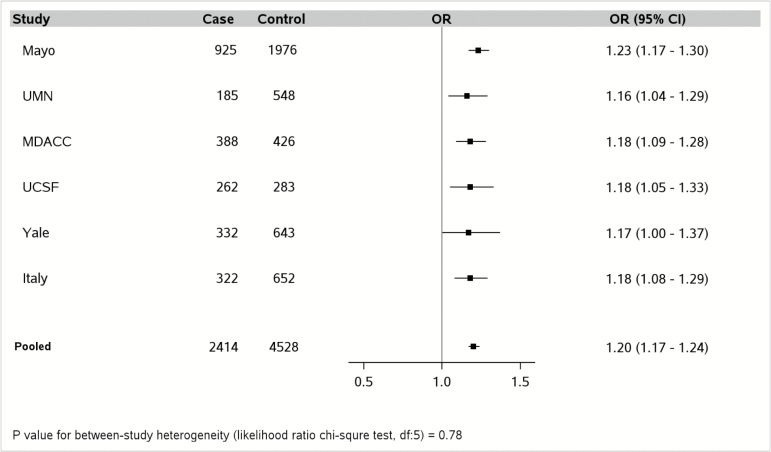
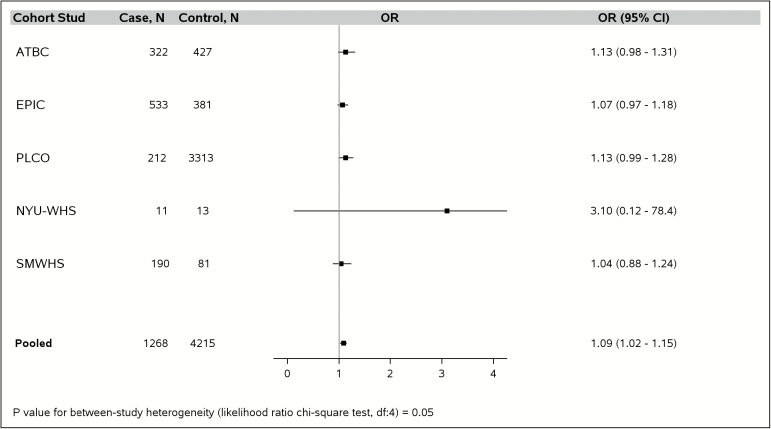
Diets with high inflammatory potential are suspected to increase risk for pancreatic cancer (PC). Using pooled analyses, we examined whether this association applies to populations from different geographic regions and population subgroups with varying risks for PC, including variation in ABO blood type. Data from six case-control studies (cases, n = 2414; controls, n = 4528) in the Pancreatic Cancer Case-Control Consortium (PanC4) were analyzed, followed by replication in five nested case-control studies (cases, n = 1268; controls, n = 4215) from the Pancreatic Cancer Cohort Consortium (PanScan). Two polymorphisms in the ABO locus (rs505922 and rs8176746) were used to infer participants' blood types. Dietary questionnaire-derived nutrient/food intake was used to compute energy-adjusted dietary inflammatory index (E-DII®) scores to assess inflammatory potential of diet. Pooled odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using multivariable-adjusted logistic regression. Higher E-DII scores, reflecting greater inflammatory potential of diet, were associated with increased PC risk in PanC4 [ORQ5 versus Q1=2.20, 95% confidence interval (CI) = 1.85-2.61, Ptrend < 0.0001; ORcontinuous = 1.20, 95% CI = 1.17-1.24], and PanScan (ORQ5 versus Q1 = 1.23, 95% CI = 0.92-1.66, Ptrend = 0.008; ORcontinuous = 1.09, 95% CI = 1.02-1.15). As expected, genotype-derived non-O blood type was associated with increased PC risk in both the PanC4 and PanScan studies. Stratified analyses of associations between E-DII quintiles and PC by genotype-derived ABO blood type did not show interaction by blood type (Pinteraction = 0.10 in PanC4 and Pinteraction=0.13 in PanScan). The results show that consuming a pro-inflammatory diet and carrying non-O blood type are each individually, but not interactively, associated with increased PC risk.
© The Author(s) 2018. Published by Oxford University Press. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures

References
-
- Jemal A., et al. (2011)Global cancer statistics. CA. Cancer J. Clin., 61, 69–90. - PubMed
-
- Antwi S.O., et al. (2017)Cancer of the pancreas. In Thun M. Linet M.S. Cerhan J.R. Haiman C.A. and Schottenfeld D (eds) Cancer Epidemiology and Prevention, 4th Edition Oxford University Press, New York, pp. 611–634.
-
- Siegel R.L., et al. (2017)Cancer statistics, 2017. CA. Cancer J. Clin., 67, 7–30. - PubMed
-
- Raimondi S., et al. (2009)Epidemiology of pancreatic cancer: an overview. Nat. Rev. Gastroenterol. Hepatol., 6, 699–708. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 CA082729/CA/NCI NIH HHS/United States
- BHF_/British Heart Foundation/United Kingdom
- UM1 CA182934/CA/NCI NIH HHS/United States
- R01 CA070867/CA/NCI NIH HHS/United States
- R01 CA098870/CA/NCI NIH HHS/United States
- MRC_/Medical Research Council/United Kingdom
- R01 CA098661/CA/NCI NIH HHS/United States
- R01 CA058697/CA/NCI NIH HHS/United States
- R01 CA109767/CA/NCI NIH HHS/United States
- N01RC37004/RC/CCR NIH HHS/United States
- R01 CA154823/CA/NCI NIH HHS/United States
- N01 CN045165/CN/NCI NIH HHS/United States
- R01 CA098380/CA/NCI NIH HHS/United States
- 001/WHO_/World Health Organization/International
- R25 CA092049/CA/NCI NIH HHS/United States
- P30 ES000260/ES/NIEHS NIH HHS/United States
- P30 CA016087/CA/NCI NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- N01 CN045035/CN/NCI NIH HHS/United States
- R01 CA124908/CA/NCI NIH HHS/United States
- R01 AG034588/AG/NIA NIH HHS/United States
- R01 CA098889/CA/NCI NIH HHS/United States
- P50 CA102701/CA/NCI NIH HHS/United States
- R03 CA108370/CA/NCI NIH HHS/United States
- N01 RC037004/RC/CCR NIH HHS/United States
- R03 CA089726/CA/NCI NIH HHS/United States
- R44 DK103377/DK/NIDDK NIH HHS/United States
- CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
